

Working effectively to address child sexual exploitation: Evidence Scope (2017)
Acknowledgements
Research in Practice would like to extend heartfelt thanks to Jan Webb, Principal Lecturer and Professional Lead Child Health and Welfare at Greenwich University and lead author of the original version of this scope. Her hard work and that of Charlotte Oram, Research Assistant, over many months is much appreciated.
We are thankful to busy colleagues in Wigan Council, Rochdale Borough Council and The Children’s Society for their ongoing input and passion for evidence.
Thanks also to Sue Botcherby and Sara Scott for their input and support in the first version published in 2015.
Our gratitude to Jessica Eaton who revised this scope in 2017 to reflect new evidence and practice wisdom. A labour of love indeed.
Limitations of this review
This evidence scope is not a systematic review; accordingly, the quality of each study or report was not assessed. However, it draws largely on published research, prioritising peer-reviewed literature where possible, and uses credible sources for policy literature and other sources of information. The literature used is largely recent, and, if not, then of enduring importance.
A full description of the methodology can be found in Appendix A.
This evidence scope was undertaken for the specific purpose of supporting colleagues involved in the Greater Manchester CSE Innovation Project in their efforts to redesign CSE services. As such, its purview has developed over time in response to their feedback and lines of enquiry; it does not offer a comprehensive review of all evidence related to CSE.
This revised edition, published in 2017, reflects the emergence of new evidence and practice wisdom.
This evidence scope formed one element within a range of research activities in the overall project in Wigan and Rochdale, including case file analysis, biographical interviews with young people, focus groups with staff and peer review.
The messages within this scope reflect the review team’s interpretation of the evidence.
1. Introduction
This scope aims to support local areas in the continual development of child sexual exploitation (CSE) services by reviewing and critically appraising relevant evidence. The scope proposes six key principles for effective service design (see Section 9).
Whilst this scope focusses on practice with children, it is the identification, early intervention, investigation, prevention, prosecution and monitoring of child sex offenders that will ultimately protect children. Professionals working in legal services, policing and the criminal justice system all have a critical role in reducing the abuse of children in society. The intervention and prosecution of sex perpetrators is, however, outside of the remit of this evidence scope. For those keen to explore these issues, there is an established body of empirical research, theories and practice evaluations focusing on child sex offenders and abusers in forensic psychology and criminology; in addition to practice guidance and advice for police, custodial services, probation and the wider network of practitioners.
Protecting children and young people from sexual exploitation is a challenging area of practice across all sectors, including health, education, the police and third sector organisations, as well as social care and social work. It is a sensitive phenomenon around which there is still uncertainty about how to respond, in part due to its complexity.
Although CSE may be a complex area, what is not in question is who causes CSE. The blame lies clearly with the perpetrators who exploit young people and cause them harm; this is irrespective of the behaviour or circumstances of the victim. This scope explores many factors that focus on young people, but this should not detract in any way from the fact that responsibility for the abuse lies with the perpetrator. Discussions within this scope actively challenge assumptions, practice and language that may contribute to victim blaming of children affected by CSE.
Throughout the scope we use the terms ‘young person’ and ‘young people’ as well as ‘children’. Whilst it is vital to recognise that all persons under 18 years old are children, this scope presents a synthesis of findings and issues from different fields and these tend to adopt different language. In CSE, a great deal of the literature and practice focuses on older children, as this group appear to be those most likely to be affected by CSE 1, and so often uses the term ‘young people’. The term ‘young person’ is also the preferred term used in participation (a topic which is discussed throughout this scope) and tends to be the terminology used by older children themselves. Given the imperative to challenge the notion that any child can ever bear responsibility for abuse and exploitation, using these terms interchangeably presents some difficulty, especially as the term ‘young person’ might be interpreted as conveying more agency and responsibility than the term ‘child’. However, this scope tries to convey the language used by the particular authors of each piece of evidence or research; therefore it will vary throughout.
This approach of adhering as closely as possible to the original source presents other challenges. Some research in this area has been produced in countries, or at a point in time, where terms that would now be considered inappropriate have been used (such as ‘child prostitution’ to describe child sexual abuse and exploitation). This scope takes the view that despite this uncomfortable use of language, the research findings are often valid and useful.
It is important to acknowledge that the extent of CSE in the UK is significant, and that awareness of the scale of the problem, both in the UK and internationally, has increased in recent years (Chase and Statham, 2005; OCC, 2013a). While societal awareness of CSE is increasing, the question of how best to tackle it remains a challenge, not only for social work professionals but for all practitioners across the children and young people’s workforce also.
Social workers have a statutory duty to safeguard children and young people. They are also the leads in inter-agency and inter- professional working when significant safeguarding concerns arise (HM Government, 2015a). However, tackling CSE is an issue of multi-agency responsibility. The centrality of partnership working is evident in terms of inter-agency and professional collaboration, information sharing across sectors and across geographical boundaries, and working in partnership with local communities, families and young people themselves (Laming, 2009; Munro, 2011; HM Government, 2015a).
Laming (2009: 36) highlighted that in order to safeguard children and young people from harm, relationships between practitioners are crucial:
Too often, agencies co-operate and share information with social services out of ‘good will’ rather than in recognition of their statutory duty. In any case, statutory duty is not enough on its own. In order to address CSE effectively, there needs to be a cultural shift. As the government’s recent paper on tackling child exploitation notes, what is required is:
Put simply, this is bigger than social workers.
All service providers in touch with young people and their families have a role in identifying and working with sexually exploited young people and in disrupting and prosecuting abusers (Pearce, 2014; HM Government, 2015a, 2015b; Beckett et al, 2017). Practitioners at all levels and across all agencies – as well as the wider community – must be able to recognise and respond to concerns related to the various manifestations of CSE. Clear strategies for intervention are needed, resourced at both an operational and strategic level, together with an approach that enables integrated working.
This evidence scope is, therefore, concerned with gathering evidence that supports interventions and multi-agency and inter- professional approaches to working to improve outcomes for young people who may be affected by CSE. Wherever possible, this includes a preventative and early help perspective. It draws on a range of national evidence and perspectives in order to provide a balanced overview for service design.
It was commissioned by Wigan and Rochdale councils, as part of the Greater Manchester CSE project, funded by the Department for Education Children’s Social Care Innovation Programme. It was revised by Jessica Eaton in 2017 to reflect new evidence and emerging practice wisdom.
Aims of the scope
This scope offers a set of principles drawing on evidence from a variety of sources to underpin the development of a new service. The main aims are to:
- Review the literature in relation to CSE
- Identify the key messages and implications for service design, practice, leadership and, where possible, commissioning
- Identify key principles to inform service developments and ways of working in practice.
This rapid scoping exercise focuses on the following key areas:
- How the problem is interpreted, defined and contextualised within contemporary policy and practice, and within society
- Issues of recognition and response
- Considerations when assessing the needs of children and young people at risk of, or experiencing, CSE
- Central tenets of effectiveness when working with these children and young people, including assessment and interventions for both the short and long-term reduction of harm, and the role of families
- The support needed for the workforce to operate effectively in this area
- Participatory approaches in practice and service design – the benefits and theoretical underpinning.
It is important to emphasise, however, that this is not a systematic review; the literature is too wide ranging and no scientific approach has been applied to assessing the reliability and validity of any research findings referred to. However, the scope does draw on peer- reviewed published research where possible, thereby offering a degree of assurance regarding the validity of the data. The scope does not include: international direct comparisons; case studies from primary research; the views of parents, families and young people 2 (other than those reported in the existing literature). While there has been considerable media interest in the issues of CSE, detailed analysis of media reports is outside the remit of this work.
A more detailed overview of the methodology is detailed in Appendix A.
2. Background and context
This section outlines definitions, provides the contextual background and historical contemporary perspectives, and defines the ‘problem’ within the current UK context in order to inform understanding of recognition and responses to CSE. Subsequent sections will focus on identification, assessment, interventions and young person-centred approaches to developing services.
2.1 Definitions
Definitions provide the conceptual framework for practice within which legislation, policy, data collection and research are located. Whilst the definition of child sexual abuse (CSA) has remained fairly stable for a long period of time, the definition of child sexual exploitation (CSE) has been in a state of evolution in recent years. Currently, the definitions draw a distinction between CSE and CSA, so each one will be discussed here.
Looking at policy definitions, the government’s guidance Working Together to Safeguard Children states that sexual abuse:
The definition of CSA provides detail of abuse and offence types and also seeks to break down some important assumptions within it. It should be noted that the definition of CSA clearly positions the abuse as harmful and illegal. It makes sure that CSA can be defined without the presence of other physical violence and also states that the child may or may not know what is happening to them. The final sentence is also a reminder that perpetrators of CSA are not always male, an important point in light of evidence suggesting female child sex offenders are under-identified (Elliott, 1995).
The terminology used in relation to CSE (and its definition) has been in a state of flux for some time. This recently underwent further iteration in February 2017 with the government publishing a new definition (see below). The abuse now known as CSE has been written about since at least 1856 (Hallett, 2017) and terminology has come a long way since the term ‘child prostitution’ which was used widely until pressure from feminist and child rights organisations meant that the term came under increasing scrutiny. It was briefly changed to ‘abuse through prostitution’, then ‘commercial exploitation’ of children and, now, ‘child sexual exploitation’. Practice terminology and legal definitions were not adapted in tandem, however; until 2015 the Sexual Offences Act 2003 still used the term 'child prostitution'.
This offers some insight as to why the definition of CSE now looks rather different from the definition of CSA, despite CSE unarguably being a form of child sexual abuse. This evolution could also offer insight into the sticky concept of ‘exchange’, which is discussed further below. A further criticism of the evolving language around CSE is that it is becoming ‘hygienic’ and abstract, whereby the definition does not represent the true harm, violence, injuries and death of children, but describes a vague process of exchange with no reference to harm or trauma (Gladman and Heal, 2017).
Just as the terminology has been evolving, so too has the definition of CSE. There has been debate as to whether a definition of CSE is needed, especially now that the new definition states firmly that CSE is a form of CSA (Shuker, 2015). In February 2017, the government issued a new definition of CSE:
The statutory definition is now applied and is considered the main definition of child sexual exploitation 3. Previously there have been a number of different definitions of CSE, including definitions written by The Children’s Society, Department for Education, Association of Chief Police Officers and the NWG (formerly The National Working Group for Sexually Exploited Children and Young People).
Until the change in February 2017, this is how the NWG defined the sexual exploitation of children:
The definitions of CSE and CSA look very different and may be subject to further change and evolution as the evidence base matures. A key distinction explored by Beckett and colleagues in the ‘extended text’ 4 of the national CSE guidance (Beckett et al, 2017) is that CSE involves a power imbalance and an exchange of something ‘tangible or intangible’. However, it is important to note that CSA always occurs with a power imbalance (and this is included as a footnote by the authors); but what about the exchange? Recently, survivors from Rotherham have been challenging the notion of ‘exchange’ by arguing that the concept is offensive to victims and survivors because it reframes the violence and abuse as reciprocal (Woodhouse, 2017). It can be argued that CSA involves some form of exchange, especially that of intangible exchange such as being made to feel special, keeping an important secret, buying toys, or being treated better (or worse) in order to keep the child from identifying, understanding or disclosing their abuse to someone else. This point is also acknowledged by the authors and others, who note the concept of exchange is not unique to CSE and that the definition has become too vague (Shuker, 2015). A critical point is that despite ample evidence that exchange is used by child sex offenders as a method of grooming, the receipt of goods, gifts or money has led some to consider that a child may be more complicit or consenting in cases of CSE than in CSA cases, where the child is more clearly seen as a victim and the exchange is more clearly seen as a method of grooming and control. This tension, wherein acknowledging the exchange dynamic can lead to a less protective response, is arguably not a definitional one but an educative one (Beckett and Walker, forthcoming).
In practice, this difficulty means that many cases of CSA could be defined as CSE and many cases of CSE could equally be defined as CSA. Whilst there is some benefit to exploring the distinctive elements of CSE, it is also argued that the creation of a definition of CSE, as the only legislated sub-category of CSA, can fuel an unhelpful dichotomy between CSE and other forms of CSA (Beckett and Walker, forthcoming). The importance of those definitions and perceptions of each of the terms becomes more obvious when we begin to explore the responses to these two different yet connected types of abuse.
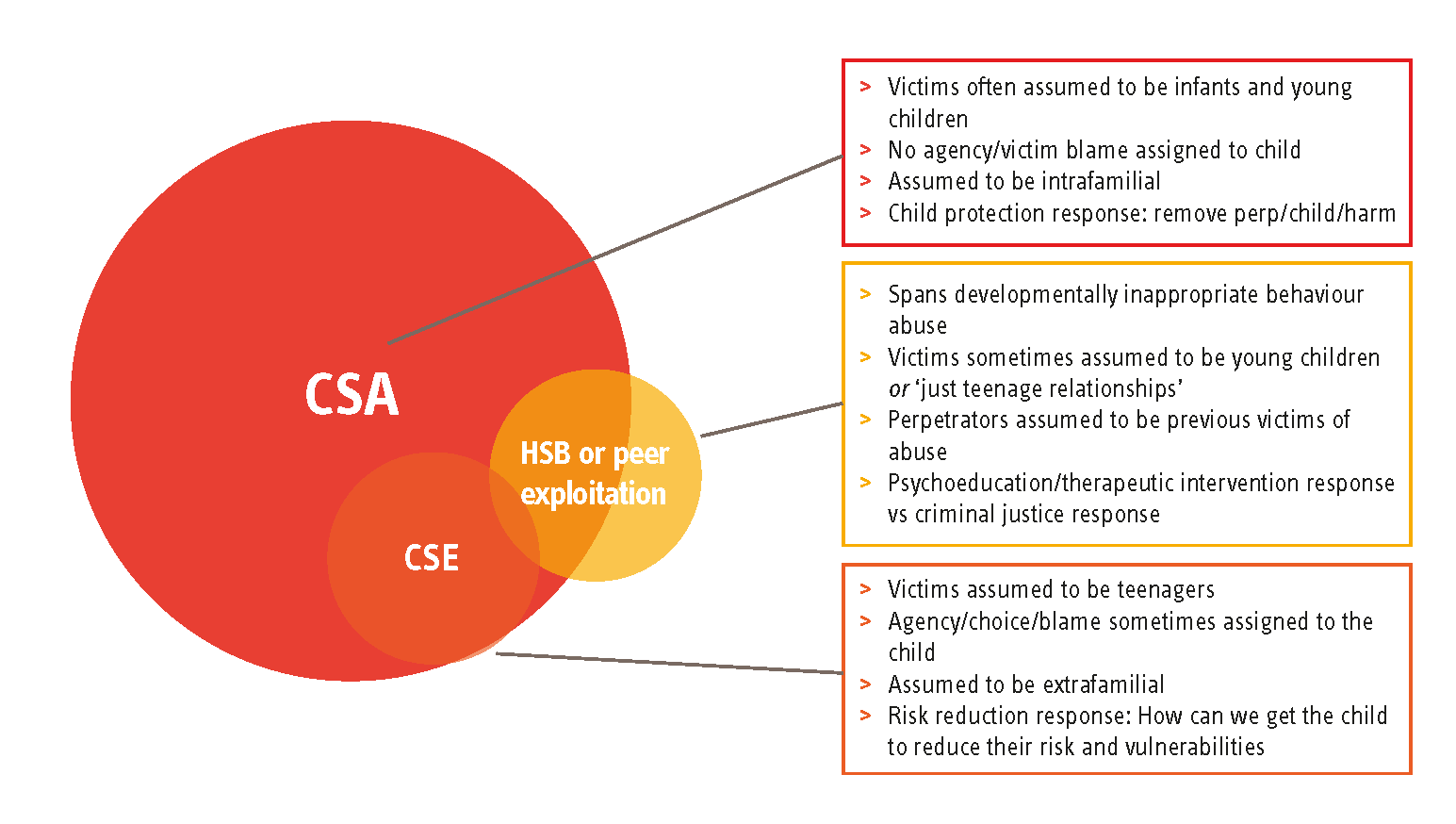
Figure 1.1: CSE and HSB as a type of CSA (Eaton, 2017)
Figure 1.1 presents CSA as the overarching form of sexual abuse within which harmful sexual behaviours (HSB) or peer exploitation and CSE exist and overlap. It is important to note that some evidence asserts that most CSA is intrafamilial, with 90 per cent of victims being sexually abused by someone in their family or close support network5 – though such estimates are challenging due to the hidden nature of sexual abuse and the changing perceptions of exploitation and HSB. HSB spans a spectrum of behaviours from developmentally inappropriate through to abusive (Hackett, 2014).
Child abuse, specifically harm to younger children within the family context, is arguably the construct on which the child protection system, procedures and policies were built (Bilston, 2006). When practitioners, authorities and the general public talk about CSA, there is a general assumption that it affects small children and infants within their familial home, usually being perpetrated against by a male family member. The response is often swift and aims to remove the child from all harm to a place of safety. It is unlikely that young children who have been sexually abused by an adult family member would be blamed or assigned agency in their abuse.
Child sexual exploitation, having evolved from all of those definitions and terminology – and subject to high-profile media coverage of particular cases – tends to conjure up a very different image. Victims are assumed to be teenagers (specifically teenage girls), being exploited outside of the familial environment. Children are assigned a level of agency, choice or blame which is different to children affected by CSA, a point regularly featured in serious case reviews of child sexual exploitation (Bedford, 2015; Jay, 2014; Coffey, 2014). Some of this results in questions being asked of the child that imply blame or responsibility. Arguably, a stark difference is seen in the systemic response to the child, in which they are assessed as a ‘risk’ and then supported to reduce that ‘risk’ and/or their ‘vulnerabilities’ until the child is deemed safe. This risk reduction response places considerable responsibility within the child to safeguard themselves from further harm.
Harmful sexual behaviours and peer-on-peer abuse is different again, with HSB often assumed to be displayed by young children who have previously experienced sexual abuse and are therefore copying those behaviours with other children. Work by Hackett (2014; 2016) and others suggests a much more complicated picture. Vosmer et al (2009) and Hackett (2016) argue that not all children who abuse peers or display HSB have experienced sexual abuse and that HSB is correlated with a range of adversities such as witnessing violence in their family, isolation and environmental factors. In addition, it is important to consider emerging issues for this generation of children such as watching porn, being exposed to sexually aggressive media and the overall hypersexualisation of society which may be influencing behaviours of children (Vosmer et al, 2009). When children are displaying developmentally inappropriate sexual behaviours and/or found to be abusing other children, it can be difficult to achieve a response that balances the needs of both the child instigating abuse and the child experiencing it. In general, effective responses tend to be holistic and educative in nature, resilience-focused and are likely to include therapeutic intervention (Hackett, 2014).
To conclude, current definitions are not perfect and it is likely that they will continue to evolve for some time. It is important for practitioners to recognise the definitions of CSA and CSE, and to understand the potential distinctions between the evolving definitions; however, endless debate about what constitutes CSE could even be detrimental to practice (Beckett and Walker, forthcoming). Professionals are likely to require guidance, but this should be employed as the scaffolding that supports child-centred evidence-based responses to harm, and not as a restrictive and instructive definition which limits responses to harm and access to services.
Reflection pointers
- Are practitioners across all agencies aware of the distinction between child sexual abuse and CSE, while recognising that CSE is child sexual abuse?
- How do we know that practitioners are sure of what constitutes ‘sexual exploitation’?
- What else can we do to support practitioners to respond effectively to concerns about children when the type of sexual abuse may not be clear?
Background – The extent of the problem, incidence and prevalence
The scale of the problem has been highlighted in recent years. An inquiry by the Office of the Children’s Commissioner into CSE by gangs and groups identified 2,409 children as victims of CSE in little more than a year (OCC, 2012: 9); a further 16,500 children and young people were identified as being at risk of CSE. What has also emerged is that the risk of sexual exploitation begins earlier than was previously thought or acknowledged, with clear evidence that adolescents as young as 12 or 13 are affected by contact sexual abuse and children as young as 8 years old affected by online exploitation (Barnardo’s, 2011a; Ringrose et al, 2012; CEOP, 2007). The interim report of the OCC’s two-year inquiry into the nature and extent of CSE begins by stating:
It is difficult to gain an accurate understanding of the prevalence of CSE because, historically, many survivors have not come forward and because definitions and perceptions have changed. Furthermore, CSE is not always listed as a separate category in child protection procedures or crime reporting (OCC, 2012). A number of reports have attempted to estimate the prevalence of CSE. For example, the Department for Children, Schools and Families identified that 111 out of 146 Area Child Protection Committee districts had cases of CSE, with a higher prevalence of sexual exploitation of girls than boys (DCSF, 2009). The National Working Group found that over a 12-month period, 53 specialist services worked with 4,206 reported cases of CSE (NWG, 2010). In 2016-17 Barnardo’s alone supported 3,430 people through their child sexual exploitation direct support services (compared to 2,486 in 2015-16)6.
Sexual grooming via the internet and mobile technology is also widespread, making it even harder to assess prevalence accurately (Barnardo’s, 2011b; CEOP, 2013; Chase and Statham, 2005; Radford et al, 2011). Online threats to children and young people include the proliferation of child abuse images, online exploitation, transnational child sexual abuse, and contact child sexual abuse initiated online (CEOP, 2013). It is common to find areas in which almost all of the cases of CSE involve online exploitation and online grooming (Palmer, 2015). (The discourse around pornography and sexualisation is explored later in this section.)
Beckett et al (2017) succinctly note that while the prevalence data in CSE is generally unreliable due to low levels of reporting, it can be reliably assumed that CSE is happening in all areas of the UK and online.
Research in forensic psychology has been exploring what the evolution of the internet has meant for child sex offenders. O’Connell (2003) suggested that the internet has increased accessibility, vulnerability and opportunity. The literature includes exploration of offence types, behaviours and victims of online sexual exploitation. An important study by Whittle et al (2013) synthesised evidence from a range of studies. It showed online sex offenders varied widely in their grooming processes and techniques, had different goals (contact-driven or fantasy-driven offending) and that 77 per cent of sex offenders used a range of simultaneous communication methods to manipulate their victims, such as email, text, social media and phone calls.
Reflection pointers
- How do we know that our data, and that of neighbouring local authorities and partner agencies, is sufficiently accurate to identify need and plan service responses?
- How, if at all, do we capture the scale of online exploitation?
- What could be done to build better local evidence of the scale, types and impact of online exploitation?
Tackling CSE: what does success look like?
As a form of child sexual abuse, child sexual exploitation has a largely similar impact to CSA in terms of the symptoms, behaviours and harm it causes. In theory, therefore, success in ‘tackling’ CSE should look much the same. There are some considerable differences, however. Many cases deemed to be CSE include one or more abusers who is/are external to the family home and who can sometimes be difficult to identify. Practice responses to CSE commonly include the decision to remove a child from their family environment (Beckett, 2011a) because an external sex offender is abusing them; this is framed as the child being removed for their own safety and wellbeing, despite the family environment itself not being harmful. Victims of CSE are also too often met with victim-blaming responses and judgements that frame the child as ‘promiscuous’ and badly behaved (Jay, 2014; Coffey, 2014; Bedford, 2015). There are also systemic differences in the way CSE is responded to, with responses tending to follow a set of specific CSE procedures, strategies and policies.
In 2006, Scott and Skidmore conducted a commissioned evaluation of Barnardo’s CSE services. They stated that successful outcomes for children affected by CSE included increased awareness of CSE, self-protective resources and a reduction in ‘risk behaviours’ (listed as going missing and conflict with parents and carers). They argued that positive outcomes for a child would be ‘an improved ability to recognise risky and exploitative relationships’, ‘protecting themselves appropriately’ and ‘not associating with controlling/risky adults’. These outcomes were then published to guide strategic leaders and practitioners towards what a CSE service should be aiming for.
However, whilst some of these outcomes would be of benefit to any child, the evidence base and practice wisdom has changed since 2006. Accordingly, greater attention is now paid to ensuring that language does not inadvertently contribute to children being ascribed responsibility or blame. In this spirit, it is valuable to reflect on and critique the way that language such as ‘protecting themselves appropriately’ and ‘not associating with controlling/risky adults’ and ‘reducing risk-behaviours’ can serve to position the child as both the source of the problem and the source of the solution.
In light of this approach, the successful outcomes of ‘tackling CSE’ are now being described in developing local CSE strategies and organisational statements. These include educative work with the whole child population, swift identification and reporting, disrupting and removing the source of risk (the sex offender) and supporting the child with their psychological, practical and social recovery, including building resilience, processing their trauma and re-empowerment after a period of serious harm. Barnardo’s recently developed 10 year CSA strategy moves clearly towards ensuring that activity to protect children; centres on trauma informed approaches, working systemically with the adults and systems to address harm and crucially ensuring that young people have agency and that their voices lead the support process. (Barnardo’s, forthcoming).
When determining safety-focused outcomes, the work of Shuker (2013a) is useful in its argument that physical, relational and psychological safety are all vital for safeguarding the welfare of young people affected by CSE.
Tackling CSE: some of the challenges
What is clear then is that currently, CSE is not an easy issue to tackle. Moreover, young people do not always understand that they are being abused or exploited (DCSF, 2009; Beckett et al, 2017), a further challenge for those seeking to identify and address CSE (see the discussion on disclosure in Section 4). Whilst to some extent this reflects childhood naivety and the general vulnerability of being a child researchers point out this lack of understanding and knowledge is even more profound for children with learning disabilities (Franklin et al, 2015) – it would be an oversimplification to ascribe low levels of self-identification and disclosure to children’s lack of awareness alone. Adults who are being sexually abused or experiencing domestic abuse also find it hard to understand what is happening to them and to identify or label their experience as sexual abuse or rape. Children are not the only ones who struggle to identify and name their experiences; we shouldn’t expect them to be able to do so if research shows that adults also find it difficult (Miller et al, 2007; Heath et al, 2011).
While there is increasing awareness of CSE and the individual, family, societal and environmental factors that increase a young person’s vulnerability, there is a dearth of evidence for social workers and the wider children and young person’s workforce in the UK to support effective service delivery (Brodie et al, 2011; Barrett et al, 2000; Dodsworth, 2014). It is also the case that too many services have failed to respond to recommendations set out in statutory guidance, despite sexual exploitation being one of the many key problems facing young people who may already be known to services (Pearce, 2014; Ofsted, 2014; HM Government, 2015b).
As noted, challenges also stem from the fact that the child protection system itself was designed with young children experiencing harm within the family in mind (Bilston, 2006). It is therefore arguably not always helpful as the dominant construct for addressing contemporary adolescent risk (Hanson and Holmes, 2014). There is a need for greater exploration and research around the correlates and contexts of CSE, and the appropriateness and adequacy of existing child protection procedures alone to address CSE is under scrutiny (Chase and Statham, 2005; Hanson and Holmes, 2014).
A strong example of this issue is presented by PACE (2014) who published The Relational Safeguarding Model in response to the criticism that the child protection system is inadequate when dealing with CSE. One of the core arguments is that the child protection system and theory assume that the root cause of the problem lies within the child, the home or the parenting. So when CSE is perpetrated by an external sex offender, the child protection system (and those trained within it) can erroneously search for reasons and causes of the abuse within the child, home or parenting.
There is consensus in the literature that the problem requires practitioners to take an integrated and coordinated approach to the resourcing, investigation and management of CSE, at a national and local policy, practice and strategic level (Department for Education, 2012; Dodsworth, 2014; Pearce, 2014). However, this kind of multi-agency safeguarding approach at all levels can be challenging, and resource pressures in some areas are making it yet more difficult to achieve (Baginsky and Holmes, 2015). The challenges of establishing shared data sets across agencies are well documented, not least for Local Safeguarding Children Boards (Baginsky and Holmes, 2015) who have been expected to play a leadership role in developing a strategic response to CSE. These challenges may equally affect the ‘flexible’ local multi-agency arrangements for safeguarding that will replace LSCBs 7 . Added to this is the challenge that CSE spans geographical areas, so the lack of clarity and consistency in data gathering creates challenges for effective analysis and triangulation across borders. Despite these challenges, police forces have been working together to develop intelligence recording systems and intelligence sharing protocols (such as Operation Striver 8) so that information held on victims is also shared across police force areas, rather than remaining the sole information of one force. When children are being trafficked during sexual exploitation, the sharing of information across force borders is vital.
There is much to learn from assessing the literature and exploring the more effective elements of service responses – as this scope seeks to do. However, there is no one gold standard model for service design and delivery.
Reflection pointers
- How do our information-sharing protocols and data collation systems between agencies enable consistency, comparison and triangulation?
- How do we capture what is working in relation to local CSE responses (and why it is working) in order to build our evidence base?
- What is being done to ensure that local innovation is grounded in evidence, and that learning from implementation is captured?
Key messages
- Local areas need to use local data and local knowledge along with available evidence from research, theory and practice, to design a service response that best meets local needs while also addressing national agendas and policy.
- Effective data collation and sharing protocols between agencies and between areas is vital to identify need and plan responses.
- A continuous evaluation and audit cycle built into services is vital in order to build knowledge of what is effective.
- Service design and delivery needs to take into account the particular needs and circumstances of young people locally, rather than follow rigid models.
- There is no gold standard model for service design and delivery. Nevertheless, there is much to learn from assessing the literature and exploring the effective elements of service responses.
Historical perspectives and their influence on contemporary approaches
Although recent high-profile cases such as Operation Span, Operation Retriever and Operation Bullfinch in 2012-13 9 have brought CSE squarely into the public domain, CSE is not a new phenomenon (Coffey, 2014). Hallett (2017) provides evidence that CSE was being discussed – and being clearly identified as the sexual exploitation of children – in 1856 by writers who were concerned that ‘child prostitutes’ were really being abducted, used and raped. CSE was later framed within arguably narrow salvationist, paternalistic and welfarist approaches and concepts of child (sexual) abuse, stranger danger, ‘child prostitution’ and grooming (Melrose, 2013; Hallett, 2013; Cockbain et al, 2014). As was once the case with other models or definitions of child abuse, the existence of CSE as a specific concern has been hidden or denied (Corby, 2006; NSPCC, 2013a). This is significant because concerns can only be tackled when there is acceptance that a problem exists. Acceptance of the problem needs then to be followed by a shared definition of that problem, accompanied by strategies, systems and policies to address it.
Until the 1990s the main child protection concerns were with intra-familial abuse (primarily physical, sexual and emotional abuse) and neglect. Concerns then began to emerge about extra-familial abuse, including organised sexual abuse and ‘child prostitution’. This shifted and extended the focus of practice, but practice has attempted to evolve within the confines of the original definitions of child protection. The period from the mid-1990s to 2008 can be seen as a time when policy shifted from a narrow child protection focus towards a more family and child-focused orientation (Gilbert et al, 2011).
Parton (2014) argues that in order to ensure systems work – both to safeguard children and young people more widely and to respond to those who need protection from harm – policy and practice must have a children’s rights perspective at their core. Such a perspective recognises that there are a wide range of significant and social harms that cause or collude with child abuse and maltreatment, and many of these are clearly related to structural inequalities (Bywaters et al, 2017). Featherstone et al (2014) have contributed to this debate, challenging the ethics and values of an authoritarian approach with multiply deprived families, and urging a shift in child protection practice and culture in order to recognise children as relational beings.
The existence of child abuse in history, including both CSA and CSE, is indisputable; what remain contentious today is the extent of CSE and its interpretation. CSE now has a high profile. It generates considerable concern within communities and has led to multiple policy and professional initiatives (Barnardo’s and LGA, 2012; OCC, 2013a; Department for Education, 2012; Department of Health and PHE, 2015; HM Government, 2015b; NSPCC, 2013b; Royal College of Nursing, 2014; Pearce, 2014). As with child sexual abuse, CSE has been a difficult subject to talk about and therefore difficult to address (NSPCC, 2013b). It was not until the late 1990s that UK governments and policymakers gave CSE due attention. Until recently, different models of exploitation were contextualised as other forms of child maltreatment or located within ‘child prostitution’ as child protection concerns (Pearce, 2009a). Significantly, the OCC’s inquiry into CSE in gangs and groups (OCC, 2012) recommended that use of the term ‘child prostitution’ should be removed from government documents and strategies and from legislation. Coffey (2014) further recommended there should be no references to child prostitution in any legislation (see also Barnardo’s, 2014b: 11). They have succeeded in this, achieving much more than simply a shift in language but arguably prompting also a shift in attitude. Language matters; it both reflects attitudes and can form attitudes. Just as with the now widely criticised term ‘child pornography’, when child abuse is erroneously conflated with adult activities we risk inferring consent from, and blame towards, the child victim.
Despite this increased attention, however, some uncertainty about what constitutes CSE remains (Melrose, 2013). How CSE is defined or interpreted is in turn related to wider issues in society. And although the problem is not actually a new phenomenon, there is some newness to the issues that surround it. For example, new technologies and media provide easier access to pornography, not only providing new tools for perpetrators to exploit and abuse young people, but arguably shaping young people’s perceptions of sex as well (CEOP, 2013). So in the context of CSE, there is a genuinely ‘new’ element to a long-standing but only recently recognised phenomenon; this brings new complexities and challenges for practice.
Key messages
- Concerns can only be tackled when there is acceptance that a problem exists. Historically, as with other forms of child abuse, denial and ‘blind spots’ to the existence of CSE have contributed to the challenges of defining and addressing CSE.
- Language matters; it both reflects and can inform attitudes. The use of inappropriate language can act as a significant barrier to protecting young people from CSE.
Contemporary conceptualisations
Contemporary conceptualisations, borne out of historical perspectives but advanced by recent research and developments in practice, recognise that although CSE is a form of child abuse, it is helpful to understand the many factors that contribute to the existence of and misunderstanding of CSE. When considering how best to configure a service response, it is important to reflect on a number of different perspectives and factors. These include societal reactions to the increased concern around CSE, the role of power and gender, and the ways in which risk and choice are conceptualised. Online abuse and pornography are also considered.
Media coverage and myths
The recent media attention around CSE has implications both for contemporary understanding of CSE and responses to it. When amplified by media representation, public outrage, however understandable, has the potential to do harm, not least in its impact on the workforce – as Jones notes in his discussion about the response to Peter Connelly’s death (Jones, 2014). At times of widespread public outrage, there is a need to be alert to discourses and the language used by politicians, public leaders, the media and professionals. This is significant because it is often the young person who is demonised and their behaviour seen as criminal, when in fact they are the vulnerable and exploited victim (see, for example, the serious case review authored by Bedford, 2015).
Another impact of widespread media coverage of CSE is the development of stereotypes – the more times a story is reported or told in a specific way, the more likely it is that the general public and professionals will absorb a stereotype of offenders, victims and abuse typologies (Flowe et al, 2009; Shaw et al, 2009). An example is the significant public misconception that CSE offenders are Pakistani males, which overlooks the complex picture of child sexual abuse. Perpetrators and victims of CSE are known to come from a variety of social, ethnic and cultural backgrounds and CSE occurs in both rural and urban areas (LGA, 2014). It is argued that the national media have paid considerably less attention to cases involving groups of white British perpetrators, even when the crimes and sentences are strikingly similar (Operation Kern vs Operation Retriever 10). For victims, it has meant the development of an impactful stereotype of a young white girl, generally in local authority care, known to multiple services and with overt vulnerabilities and ‘promiscuous’ behaviours (Fox, 2016). If professional resources (such as films, posters, websites and support materials) echo these victim and perpetrator stereotypes, this can exacerbate stereotyping. When it comes to abuse typology and grooming methods, the media have employed words like ‘sex gangs’ and ‘child sex slaves’ and ‘paedo gangs’ – meaning that the media have created a stereotype of organised crime gangs of paedophiles (usually this word is being incorrectly used in place of ‘sex offender’ 11) using children in a highly organised manner as sex slaves. This is a far cry from the real types of case that workers in the UK are holding; according to some researchers, only eight per cent of sex offenders abuse children with another offender (Brayley and Cockbain, 2012).
Conversely, for local areas seeking to address CSE, the increased media attention might also present an opportunity to strengthen efforts to raise public awareness and increase understanding. To realise these potential benefits, information must be accurate, free of bias and must not perpetuate unhelpful or damaging stereotypes, not just of children but also of perpetrators and offences. Careful attention must be paid to the way any kind of media reporting, awareness raising, resources and films are developed so these stereotypes do not continue to lead to blind spots and gaps in responses.
Myths around CSE
As discussed above, insensitive, inaccurate or over-simplified media stories can also play a part in sustaining myths around CSE. In addition to the myth that CSE only involves certain ethnic cultural communities, other myths also prevail, so it is especially important that practitioners are aware that:
- CSE is not exclusively about adults abusing children – there is increasing concern around peer-on-peer abuse and the risks that young people face within their own social settings, such as schools (Firmin, 2013).
- Both males and females are abused through CSE – similarly, both males and females are perpetrators.
- Perpetrators may be previous or current victims themselves.
- CSE can take place online and offline or both. Sex offenders can also groom and exploit exclusively online without any intention of ever meeting the child – online grooming should not necessarily be seen as a precursor to contact offences.
- CSE can be perpetrated by individuals or by groups.
- There is no typical CSE case; CSE takes many different forms.
- Children who are sexually exploited do not always have some sort of underpinning vulnerability; looking for evidence of the ‘vulnerability’ that ‘caused’ the sexual exploitation can lead to (or collude with) victim blaming.
- Sex offenders do not always seek out opportunities to abuse vulnerable children, they create new opportunities to abuse and they create new vulnerabilities that did not exist before.
Traditionally, perpetrators of CSE have been depicted as strangers who appear threatening and dangerous. This perception is inaccurate (Lalor and McElvaney, 2010) and can impede recognition of CSE, possibly leading to resources and interventions being misdirected to other areas of service intervention or child protection. In fact, reports show that perpetrators are often known to and indeed close to the victim; through a process of grooming and coercion, they manage to engage in sexual abuse and exploitation of the child (CEOP, 2013), which mirrors the offender types in CSA.
The notion of ‘dual identity’ in some young people affected by CSE can present particular challenges. As with harmful sexual behaviours (not specifically CSE) perpetrated by children and young people (Hackett, 2014), it is important to note that there is not always a neat distinction between victim and perpetrator. For example, the Office of the Children’s Commissioner found that six per cent of victims reported in their call for evidence were also perpetrators (LGA, 2014: 19 citing OCC, 2013a). It is also important to keep in mind that although children may appear to be willing accomplices in the abuse of other children, this should be seen in the context of the control exerted by the perpetrator. When children are being exploited by adults to recruit other children into abuse, they are still being exploited and groomed – simply for a different purpose.
Key messages
- Societal alarm and media coverage is understandable but can have unhelpful consequences, such as stereotyping and over-simplifying the issues. It can also serve to undermine professionals’ understanding and confidence.
- Societal alarm and outrage might, however, provide an opportunity for promoting greater understanding of CSE, by meeting increased public understanding and concern with accurate and informed awareness raising.
- Everyone involved in configuring, designing and leading service responses to CSE, as well as practitioners themselves, must be alert to myths surrounding CSE. It is essential that the way CSE is represented locally does not encourage or perpetuate ‘blind spots’ or simplistic stereotypes, and so place young people at risk.
- CSE is not perpetrated exclusively by adults. Young people can also be perpetrators; and young perpetrators may also be victims.
Reflection pointers
- Does any of the language used by senior staff inadvertently reinforce inaccurate or unhelpful stereotypes of CSE? For example, by ignoring female perpetrators, or by assuming there are always clear-cut distinctions between young perpetrators and victims of CSE?
- Is sufficient attention being paid locally to CSE perpetrated by peers?
Power, gender, pornography and sexualisation
As we saw in our discussion of definitions, it is currently argued that what differentiates CSE from other forms of abuse is the concept of ‘transactional sex’ or ‘exchange’ of sex for money, goods or something else (Beckett, 2011b). For the child, this means receiving or believing they will receive something they want or need, or something they think they want or need (Beckett et al, 2017). The suggestion that the child may ‘gain’ something from this transaction may be misinterpreted by adults and serve to disguise the power imbalance in play between perpetrator and victim (Beckett and Walker, forthcoming), which is arguably more readily recognised in all other forms of abuse. The concept of exchange (which, as noted previously, is contested by some) creates a particular power imbalance in the relationship, which in itself is exploitative and unhealthy for the young person, and can create an illusion of reciprocity in the minds of young people and in the minds of practitioners. The power that perpetrators wield over victims can be extremely potent (Bedford, 2015) and may not be recognised by practitioners, further heightening risk. Professionals must be conscious of this relative power when seeking to engage young people in help (RCGP and NSPCC, 2014).
There are a number a ways in which children and young people are exploited that raise uncomfortable issues about adult power and responsibility, including those relating to how the power of professionals can be experienced by victims and families. There are stark examples of practitioners not fulfilling the duties that come with occupying powerful positions (Bedford, 2015; Jay, 2014). There are also examples where relative power and status between different professional groups is said to have contributed to CSE not being addressed (Casey, 2015). Power is significant also in how families of CSE victims experience support. There are those who argue that current child protection practice and culture ignores, or exacerbates, the relative powerlessness of families who are often already experiencing multiple manifestations of disadvantage (Featherstone et al, 2014). Given that the child protection system remains the dominant construct for addressing CSE, and in light of the sense of powerlessness that parents of CSE victims report, it is important to consider whether practice with parents is intensifying this power imbalance. Recent work published by the Centre of Expertise for child sexual abuse draws further attention to this issue. According to an evidence scope 12 exploring the support needs of parents of sexually exploited children and young people, statutory safeguarding procedures and practice can make parents feel excluded, overlooked and even blamed (Scott and McNeish, 2017).
Reflection pointers
- As service leaders and practitioners, how do we talk about power? Are we sufficiently aware of our power and how it affects others?
- Do we have a shared understanding of where power rests in the ecology of CSE?
- How are practitioners supported to reflect on the notion of power in their practice with children who have been or are being exploited and their families?
Sex and gender roles
Connected to notions of power, the issue of gender is also important. Indeed, the power imbalance that occurs through sex inequality is particularly pernicious because of the long human history and culture of women and girls being oppressed and controlled because of their sex under the guise of ‘gender roles’ (Yi, 2015). As we have already noted, boys are also exploited and women can be perpetrators, often having been victims themselves (Stevenson, 2014), so simplistic assertions around sex and gender roles are not helpful. However, an analysis of sex and gender roles offer a very significant contribution to developing practice and service responses and it is important to acknowledge that CSE is, unarguably, linked to male violence against females.
The ways in which women and girls experience greater inequality, hardship and harm than their male counterparts are myriad. It is outside the remit of this scope to explore the wider cumulative disadvantages that women face across the life course (for a comprehensive review of women and girls at risk, see McNeish and Scott, 2014) but it is worth noting that the heightened risk of violence and abuse facing women is in the context of lifetime inequalities. Domestic abuse research illustrates the high prevalence of sex-based oppression and violence, with one in four women in the UK experiencing partner-perpetrated physical violence (Guy et al, 2014). As Williams and Watson (2016) note, the physical and sexual abuse of women and girls are widespread phenomena and can be seen as a way of establishing and sustaining male dominance – both within the family and community – or maintaining masculine identity (WHO, 2013). Accordingly, it is within the most male-dominated families, sub-cultures and coercive contexts – including trafficking and gangs – that some of the most severe abuse of girls and women occurs (McNeish and Scott, 2014). Research carried out for the NSPCC in 2009 found that one in three 13 to 17-year-old girls in an intimate relationship had experienced some form of sexual violence from a partner (Barter et al, 2009), while a later analysis of data from the Adult Psychiatric Morbidity Survey found one in 25 of the UK population (80 per cent of whom were women) had suffered ‘extensive physical and sexual violence, with an abuse history extending back to childhood’ (NatCen, 2014: 1). The prevalence of intimate partner violence in young people’s relationships varies depending on the type of abuse and the definitions used, according to Barter’s review of recent studies (Research in Practice, 2016a). Clearly the scale of violence towards females is vast, and CSE connects to sex-based oppression and violence both materially and conceptually.
Some years ago, Kelly et al (1995) argued the increased awareness around sexual exploitation that has now emerged is, in part, the outcome of a strong feminist movement (alongside other influences – see Finkelhor, 1979, and Kelly, 1988). They further argued that the ‘knowledge explosion’ seen during recent decades reveal significant insights:
- that males are the vast majority sexual abusers of children
- that children are most likely to be abused by a male that they know
- that abuse takes a range of forms, occurs in varying contexts, and within a diversity of relationships
- that individuals and agencies have frequently failed to respond appropriately to cases of sexual abuse, often blaming the victim and excusing the offender
- that these findings are echoed in the knowledge developed over the last 20 years [i.e. 1975-1995] about male abuse of women.
(Kelly et al, 1995: 10)
The way in which victims of CSE are perceived and treated by services is also affected by an understanding (or lack of understanding) of sex inequality. The link between abuse and mental health problems in women has been documented over many years (Chen et al, 2010) and there are lessons from research in this field that may be useful in relation to CSE. Williams and Watson (2016) highlight the risk that a woman’s response to harmful experiences – borne out of structural inequality – may be pathologised. In expressing her distress, a woman is perceived as overreacting, hyper-emotional or hysterical (Cretser et al, 1982, note historical mental health practice in which women were sectioned and imprisoned for showing emotional distress) and so the service response can be to medicalise, diagnose and situate the problem within the woman.
A contemporary example of this phenomenon comes from medicine. Studies have found that women in A&E departments waited longer, were given fewer painkillers and were deprioritised compared to men expressing the same levels of pain (Hoffmann and Tarzian, 2001; Chen et al, 2008). The analysis of these findings includes the suggestion that medical professionals are affected by sexist stereotypes and see women as hyper-emotional and more irrational than men, and more often perceive women’s physical pain and illnesses as psychological issues (in comparison to those of men). The lived experience of pain and trauma in females is thereby downplayed, as are the inequalities underlying their experience (Williams and Keating, 2002, cited in Williams and Watson, 2016). Females experiencing abuse express their distress in many ways, some of which may be construed as problematic to professionals but may in fact be a form of resilience or survival tactics. By focusing on the expression of pain rather than the harm and inequalities that enabled it, and by comparing this with what women and girls who conform to gender role do, there is a risk not only of failing to address the issue, but of locating fault within the victim also.
The powerful connections between a woman’s distress and her lived experience are severed and without these understandings, her rightful distress and associated struggles to survive are easily misunderstood as abnormal, dysfunctional, unhealthy, out of control or dangerous. It becomes easy to assume that there is something fundamentally wrong with her, rather than that something has gone badly wrong with her life.
(Williams and Watson, 2016)
If we reflect on how young women experiencing CSE can sometimes be treated by services – for example, being described as ‘wild’ or ‘out of control’ or placed in secure settings, which may be experienced as punitive and can be counter-productive (Creegan et al, 2005) – then sobering parallels can be drawn with the picture described above. It is vital, therefore, that practitioners, service leaders and policymakers recognise and respond to the ways in which sex inequality both precipitates sexual exploitation and can lead to discriminatory approaches in the very services aiming to address its impact.
Reflection pointers
- Is an understanding of sex inequality evident in our local strategy, service response and practice?
- What measures do we have in place to ensure that everyone working to address CSE is able to recognise and understand the central role of sex inequality and discrimination? Is there more we can do?
- What are we doing to ensure that our efforts to tackle CSE are effectively connected to other local activity that seeks to address violence towards women and girls more generally?
Pornography and hypersexualisation
Reflecting on sex-based oppression leads us to a discussion about pornography and the hypersexualisation, objectification and dementalisation of women and girls. Williams and Watson (2016) note that pornography has been linked to rape, domestic violence, the sexual abuse of children, sexual harassment and economic abuse. It is worth briefly considering the different perspectives around pornography and the hypersexualisation of children.
A significant proportion of children and young people are exposed to pornography (both online and offline), which can lead to an unhealthy attitude to sex and relationships (Chase and Statham, 2005; Horvath et al, 2013). Advances in mobile technology mean children and young people are able to access far more easily than was possible for previous generations; material that is considered highly inappropriate and even damaging. A study by Martellozzo et al (2016) found that 28 per cent of 11 and 12-year-olds had watched pornography and that girls and boys reported being asked to replicate sex acts they saw in porn, with one boy saying ‘My friend has started copying stuff he sees in porn with his girlfriend, nothing major, just a few slaps here and there’ (p38). Boys have also been found to be ‘collecting’ nude images of girls after asking them to write the boy’s name on their genitals or breasts with marker pens to prove ‘ownership’ (Ringrose et al, 2013). Other researchers have also found people to be developing sexual performance and intimacy issues in their adults lives due to addictions to porn and changes in the way the brain is aroused by visual imagery rather than physical stimulation (Zoldbrod, 2013; Park et al, 2016). It is also worth mentioning that pornography itself is exploitative in nature (especially for females) and therefore children and young people need open and frank discussions about the type of sex and the context of sex within pornography. Research for the Department for Education in 2011 13 found that nine out of ten parents felt their children were being ‘forced to grow up too quickly’ and to engage in ‘sexualised life’ before ready to do so. This is thought by some to be precipitated by a celebrity-driven culture as well as increasingly sexualised media programming and clothing (see Bailey, 2011), but it is important to be cautious about suggestions of simple causal or mono-directional relationships precipitating CSE. What is vital is always to maintain absolute clarity that children deserve protection, irrespective of how innocent and chaste they may or may not present – and that the problem is how children are sexualised and how this cultural sexualisation can present new opportunities for child sex offenders that may not have existed years ago. An example of this could be that talking to a child about sex, or attempting to sexualise a child during the grooming process, may be easier for child sex offenders in the current culture of hypersexualisation of children. Children are now absorbing sexualised images and messages from an early age. In 2007 an American Psychological Association taskforce found that girls begin to self-objectify and to ‘self-sexualise’ (the act of judging oneself by sexual worth and imagining oneself through the male gaze) by the age of seven. Therefore, a sex offender initiating a conversation about sex or calling a child ‘sexy’ may not be such a difficult task now as it was when discussing sex was considered taboo.
The Children and Social Work Act 2017 requires the Secretary of State to make regulations that will require ‘relationships and sex education’ (RSE) 14 to be taught in all secondary schools and relationships education (as part of PSHE – personal, social, health and economic education) to be taught in all primary schools 15.This was a widely supported and progressive move by the government, backed by children and young people themselves. (A survey of 16 to 24-year-olds carried out by the Terrence Higgins Trust in 2016 found that 99 per cent thought RSE should be mandatory in all schools; one in seven respondents said they had not received any RSE education at all.) In this context, it is important to state that RSE does not precipitate the early sexualisation or sexual activity of children (Kirby et al, 2007; Kohler et al, 2008), despite concerns that this may be so. Effective RSE can help children and young people to manage how the media seek to sexualise them and can help them promote their own agency.
However, whilst RSE is often presented as a protective factor for children and young people in the context of abuse and exploitation (Wurtele and Miller-Perrin, 1992; Rekart, 2005; Wolak et al, 2008; PACE, 2013), the evidence base is not yet mature enough to support this assertion. Bovarnick and Scott (2016) conducted a rapid evidence assessment, which focused on the effectiveness of ‘preventative education’. They were able to identify only a limited number of studies and found extremely small or zero impact of this type of input on the sexual and relationship behaviours of children. There may be evidence of temporarily increased knowledge of the topics being taught, but it would not yet be accurate or ethical to assert that education is ‘preventative’ or ‘protective’ against CSE. That said, whilst it is important that RSE or even CSE information is not labelled as a ‘preventative education’ (as it cannot prevent an abuser acting), there are clear reasons why children should have access to early, comprehensive and modern education about relationships, sexuality and health. The UN Convention on the Rights of the Child sets out in a number of its articles that children have a right to information and education about their own health and wellbeing. Furthermore, education may help to support children and young people to recognise their experiences as abusive and so may support disclosure; although the evidence base for this is very limited at present (Bovarnick and Scott, 2016). Barnardo’s has begun working alongside young people to identify what effective prevention work may look like focusing on disrupting the development of sexually abusive behaviours and supporting the development of safer environment where abusive behaviours are identified and effectively addressed, in response to the limited evidence base discussed above 16.
Notions that young people in contemporary society are more sexually active than previous generations, and at an earlier age, are often portrayed in the media as a source of concern. A positive interpretation of this may be that young people today have access to more family planning options than previous generations and have greater sex equality, which by implication means more freedoms and thus gives them choice regarding sexual behaviour (Lemos, 2009). On the other hand, a feminist perspective argues that pressure to be sexual at a younger age is actually evidence of sex inequality and results in fewer freedoms not more, especially in light of societal pressures and sexual culture (Attwood, 2006; Coy, 2008; Kelly et al, 1995).
We need to acknowledge that tensions do exist between liberty and safety. For some young people, early liberation and the desire for increased independence, coupled with (healthy and expected) reduced parental supervision, may present an opportunity for a child sex offender in their environment to target them (Ericson and Doyle, 2005; Barnardo’s, 2011a). Therefore, culturally expected developments during adolescence – such as reduced parental supervision, meeting new people, visiting new places, starting to date and starting to explore sexuality – can often be presented as ‘risks’ or ‘vulnerabilities’ to CSE, which can inadvertently problematise normal developmental changes and experiences. More recently this has led to these normal developments and positive risks sometimes being negatively reframed as ‘risk taking behaviours’ that need to be ‘reduced’ by professionals.
Key messages
- Practitioners and local policymakers need to be attuned to the availability and impact of pornography, and to provide young people with effective counter-narratives of sexuality and to discuss the exploitative truths of pornography as an industry.
- Liberty does not exacerbate risk per se. Supporting age-appropriate, positive risk is an important part of healthy child development.
- It is important that positive risks, decisions and developmentally appropriate changes are not framed as problematic or pathological in nature when considering the possibility of CSE.
- Children and young people should be afforded protection and allowed autonomy, even if they are a CSE victim themselves.
Getting the balance right is important.
Reflection pointers
- How are practitioners supported to develop their confidence and ‘literacy’ with regard to developments in social media and new technology?
- How do practitioners and services beyond those focused on CSE, including schools and youth services, challenge unhealthy sexual narratives?
- How are parents, carers and young people supported to understand adolescent development, and the associated challenge of balancing liberty and risk?
'Risky behaviour', 'choice' and other euphemisms: Victim blaming in CSE
When working with young people, the response of practitioners may reflect faulty assumptions that adolescents and other young people are more resilient than younger children by virtue of their age, despite having experienced more cumulative harm (Rees and Stein, 1999; Stanley, 2011). And as already discussed, professionals can inadvertently compound such misconceptions through their attitudes and language. Describing victims as ‘risk taking’, for example, locates responsibility in the victim; describing perpetrators as ‘lads’ (Bedford, 2015) underplays threat. The use of euphemisms and ambivalent language can allow risk to go unseen. For example, professionals might describe a 12-year-old girl as ‘sexually active’ or a 35-year-old male as a 14-year-old’s ‘boyfriend’ as opposed to an abuser (Beckett, 2011b).
As noted in numerous serious case reviews (SCRs) and inquiries, CSE is sometimes not acknowledged because the young person is seen to have engaged in ‘risky behaviour’ and/or made risky ‘choices’; therefore responsibility has been placed, implicitly or explicitly, with the young person themselves. Confusion exists around age and consent in relation to CSE; sometimes, children and young people are seen as having ‘consented’ to their own exploitation. As the Local Government Association states:
Pearce discusses this issue, noting how instead of being viewed as victims of abuse, young people (particularly those aged 16 to 18) who were being sexually exploited ‘were invariably perceived to be consenting active agents making choices, albeit constrained, about their relationships’ (Pearce, 2014: 163). This resulted in them being apportioned blame and a degree of responsibility for outcomes which diverted attention from their vulnerability and from the actions of the sex offender. When we consider this misconception against the wider backdrop of worrying attitudes towards women’s sexual safety – according to a 2009 Home Office poll (see EVAW, 2011: 5), over a third of people believe a woman is wholly or partly responsible for being sexually assaulted or raped if she was drunk, and over a quarter think so if she was in public wearing sexy or revealing clothes – then it is clear that young female victims are at heightened risk of being held responsible for their abuse.
Another complication for older teenagers may arise in relation to the recent revision of the cross-government definition of domestic abuse to include young people aged 16 and 17. Although valuable in highlighting domestic abuse among older teenagers, the definition has the potential to further obfuscate cases of CSE. For example, Pona et al (2015) relate the case study of a 17-year-old girl with an abusive boyfriend who is also sexually exploiting her. Because of her age, the girl is judged by social workers to be experiencing domestic abuse rather than CSE, a judgment that does not capture all her particular vulnerabilities and makes it more difficult to protect her. It is important to acknowledge that domestic abuse and CSE may both be present and indeed overlapping, and may require different yet connected safeguarding strategies.
Overplaying the extent to which young people are exercising informed rational ‘choices’ is a theme that emerges in many CSE-related SCRs. What can be interpreted as ‘risky lifestyle choices’ may more accurately and more helpfully be understood as (mal)adaptations to earlier trauma, or as attempts to meet unmet needs (Hanson and Holmes, 2014). For example, a young person may have low self- regard and feel worthless, and may crave love and affection. A sex offender may therefore exploit this opportunity by showing false ‘love’ and ‘affection’ in order to abuse the young person (Elliott, 1995; Finkelhor, 1984). Or a child may have developed dissociative coping strategies when experiencing harm – for example, sexual abuse in childhood – which later inhibit their ability to identify that they are being abused (for more on ‘betrayal trauma theory’ see DePrince, 2005; DePrince et al, 2012). In addition, young people might believe (possibly set against the context of prior maltreatment or neglect) that they deserve no better than their exploitative relationship (Reid, 2011). Furthermore, the capacity to dissociate from pain or negative feelings (an adaptation to earlier trauma) can inhibit a young person’s ability to recognise their own distress. Understanding how previous experiences might (for some young people) underpin behaviours is important for practitioners, and demands a more sophisticated interpretation of 'choice'.
In order to address victim blaming, it is important to explore why people may hold these common beliefs about victims of sexual abuse. There are a number of complementary and interlinked theories that attempt to explain the social phenomenon of victim blaming and the cognitive reasoning underpinning the shift of responsibility from the sex offender towards the victim. Eaton (forthcoming) uses Bronfenbrenner’s ecological model (1979) to explore in detail the wide range of empirical evidence about what contributes to victim blaming at each level of society. The main theories considered by Eaton are:
- Belief in a Just World (BJW) (Lerner, 1980) – the cognitive bias held by many people that the world is a just and fair place in which people deserve what they get and get what they deserve. Originating from religion, people believe that good things happen to good people and bad things happen to bad people, so if something bad happens (being sexually abused), there must have been something they did (or didn’t do) which meant they deserved the abuse. The evidence for this theory is wide ranging, global but inconsistent. Many theorists argue that BJW explains victim blaming; others contest this as oversimplified, as some studies have shown that BJW attitudes do not correlate with victim blaming attitudes. Beliefs that bad things only happen to bad people act as a self-preservation tactic, to protect the self from feelings of vulnerability. Accepting that the world is a random place in which random (sometimes terrible) things happen to individuals for no reason at all, can create anxiety and uncertainty in humans looking for reason and balance in the universe (Eaton, forthcoming).
- Rape myth acceptance – a collection of harmful myths and stereotypes about victims, offenders and offences which affect how the victim is perceived. Rape myths include the expectation that the victim would report immediately, would have obvious physical injuries, would not know their attacker, would adequately fight off their attacker and would want to pursue prosecution (McMahon and Farmer, 2011). Rape myth acceptance attitudes are held by between one third and half of the population 18. When rape myths coalesce they form the notion of ‘classic rape’, which is what the public and professionals are commonly used to seeing and hearing about in the media, and the ‘infallible victim’ stereotype which describes the ‘perfectly innocent victim’. When a child or adult discloses sexual abuse or assaults that do not conform to the classic rape stereotype, they are much less likely to be believed, and are more likely to be blamed for their abuse or assault (Eaton, forthcoming).
- Individualism and self-preservation theories (Burge, 1986) – ‘individualism’ refers to an ego-centric, individualistic culture in which children and adults are taught they are responsible for their own lives, behaviours, actions and consequences. This may contribute to victim blaming and has been found to contribute to the use of the word ‘responsible’ and ‘irresponsibility’ in relation to young rape and sexual assault victims in college and university settings, with students arguing that victims are ultimately responsible for keeping themselves safe and avoiding sexual attacks (Anderson, 2001). This has links to self-preservation theories in which people create distance between themselves and victims by finding differences in their behaviours or characteristics, thereby reassuring themselves that they would never be a victim of sexual violence because they wouldn’t make those same mistakes (e.g., ‘Well, I never hang around in parks so that would never happen to me’ or ‘My family and I live in a nice area so our children will never be exploited’). The impact of victim blaming is significantly correlated with future revictimisation, self-blame and mental health difficulties (Filipas and Ullman, 2006; Miller et al, 2007). For a more detailed discussion of the theoretical frameworks and socio-cultural factors surrounding victim blaming, see Eaton (forthcoming).
In CSE specifically, it is of paramount importance that children are viewed, protected and supported as victims of serious crime and not as culpable, deserving or at fault in any way. Changing the language that is commonly used – such as ‘risk-taking behaviours’, ‘vulnerabilities that lead to children being abused’, ‘promiscuous behaviours’ and ‘unhealthy choices’ – is a vital step towards reducing victim blaming of children affected by CSE. This should be accompanied by comprehensive training and information for professionals on the origins of stereotypes, biases and victim blaming narratives.
Reflection pointers
- How is choice discussed, described and understood by practitioners across services for young people at risk? Do our practice norms or service responses inadvertently imply that blame or responsibility sits with the victim?
- What steps are we taking to ensure local services and approaches do not inadvertently label young people? Is there more we could do?
Key messages
- Service leaders and practitioners need to have a strong understanding of the role played by power and inequality, and sex in particular, in relation to CSE. Practitioners need to be alert to these issues and consider the power they themselves hold in their relationships with families.
- Practitioners must recognise and challenge negative and unhealthy attitudes towards sexual activity, sexuality and gender roles, and not work simply to address behaviours. Practitioners must be alert to the influence of pornography, for example.
- Although they may sometimes appear to be making an informed choice, young people cannot and do not ‘choose’ abuse or exploitation. Recognising the underlying factors that can exacerbate risk will help practitioners understand and interpret apparent ‘choices’ and avoid the danger of apportioning blame.
- It is important to understand how earlier trauma might play a part in compounding risk for CSE. However, evidence must be applied critically to avoid reductionist or simplistic interpretations.
- Sex offenders can target 16 and 17-year-olds, not just younger children. Even when young people become young adults, they still have a right to be protected.
- There are a number of theories that may explain why children are blamed for being sexually exploited. Professionals should be supported to understand overt and covert victim blaming.
3. Vulnerability, risk and ‘models’ of CSE
Identifying CSE and risk of CSE requires an understanding of how vulnerability and risk are constructed, as well as recognition of how CSE manifests. That is the focus of this section. Intervening successfully is dependent on accurately identifying children who are deemed as ‘high risk’ of being affected by CSE (before CSE has occurred), whatever their age (DCSF, 2009). Risk is itself a contested concept, however, and is seen in different ways by different people (Smith et al, 2007). Indeed, what constitutes vulnerability and risk in the lives of young people is influenced by a variety of factors, including social, personal, political and economic factors. (The practice of assessment, including risk assessment, is explored later in Section 4.)
Vulnerability and risk
Bradford (2004) states that conceptions of vulnerability are central to the way in which risk is classified. However, the totality of a young person’s vulnerability may not always be immediately recognisable from isolated (or apparently isolated) incidents and so may not be managed effectively. This is an important consideration when looking at the effectiveness of information sharing between agencies (see Section 6).
In contemporary society, ‘children’ have tended to be seen as innately vulnerable and generally unaccountable for their lives and actions (James and Prout, 1997), while adults are usually assumed to have full independence and a complete set of citizenship rights and responsibilities. Young people do not fall neatly into either category and the assumption that adolescents – or indeed adults are independent, responsible and less vulnerable is inaccurate (Hanson and Holmes, 2014). Vulnerability itself is also difficult to measure (OCC, 2017). Research that considers how vulnerability is conceptualised in different countries has noted that, within social policy, ‘vulnerability appears simultaneously to be conceptualised broadly and narrowly with a view that all children are vulnerable, but some are more vulnerable than others’ (Daniel, 2010: 235). This perspective could also be said to be true of how vulnerability is conceptualised in the UK. Evident public animosity towards some young people, and a perceived increase in deviance among young people as a social group, adds further complexity to how their ‘vulnerability’ is seen (Squires and Stephen, 2005; Brown, 2005; Kelly, 2003).
Current discourse includes ongoing exploration of the ‘risks’ or ‘risk factors’ which contribute to a child being seen as ‘at increased risk’ of CSE. Critical reflection on this is essential, given the way that these risk factors and vulnerabilities are often used in practice to assess children. Work by Brown et al (2016) found that practitioners are currently using over 110 risk factors believed to ‘increase risk of CSE’ in children, which currently have little or no evidence base (this is discussed in more detail in the section on CSE toolkits – see Section 4).
Figure 3.1 demonstrates that experiences (risks or vulnerabilities) of the child may or may not be present, but it is only in the presence of a child sex offender that these experiences may have a relationship with CSE.
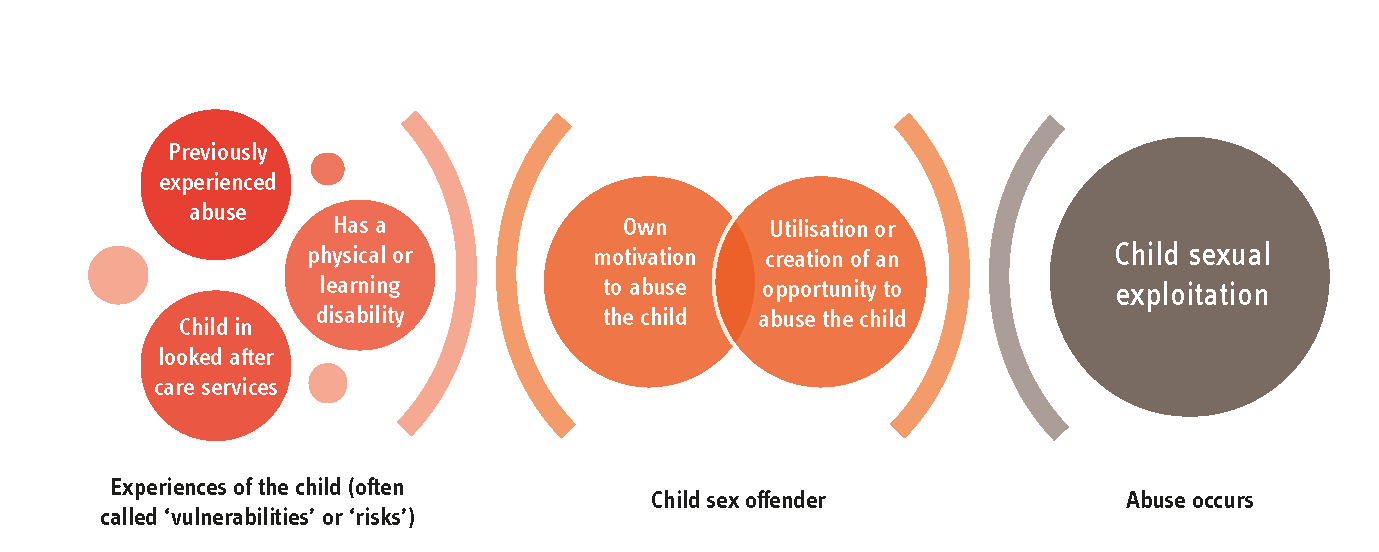
Figure 3.1: The relationship between vulnerabilities, risks and CSE (Eaton, forthcoming)
Children’s experiences may or may not be relevant to a sex offender, but research has only identified three that have any correlation with experiencing CSE – previously experienced sexual abuse (Ullman and Vasquez, 2015; Gagne et al, 2005), having a disability, and being in looked after care services (Brown et al, 2016). These are included in section 1 of the diagram.
Earlier and current literature on CSE focuses heavily on the ‘vulnerabilities’ of the child. However, whilst some children who are sexually exploited may have experienced other issues in their lives before the sex offender targeted them, it would be premature to link these as causal, or in some cases even correlational. Studies such as the Adverse Childhood Experiences (ACE) Study frequently find that over 70 per cent of adults report at least one adverse childhood experience and over 12 per cent report more than four 19.This means that, statistically, a large majority of children in the population have experienced harm or trauma, but have not gone on to experience CSE.
In Figure 3.1 the previous or current experiences of the child stand independently from the abuse process unless the child is being targeted by a sex offender. A child might experience multiple harms or vulnerabilities but will not be sexually exploited unless a sex offender targets them. If there is no sex offender, there will be no sexual offence against the child. The sex offender operates independently using their own motivations coupled with the utilisation or creation of an opportunity to abuse, which may or may not include the child’s existing experiences. This means sex offenders may know and choose to use the child’s adverse experiences to groom or control them – or they may not know (or not need to know) about any previous or current experiences, because they aim to create a new experience, such as offering drugs or alcohol, that was not already a feature of the child’s life.
In considering early childhood harm and trauma, it is also worth briefly acknowledging the work of those who argue that maltreatment in the early years may affect brain development (Child Welfare Information Gateway, 2009; Brown and Ward, 2013). It is suggested by some researchers working in this field that this may explain some impulsivity and risk taking in young people (see Hanson and Holmes, 2014, for more discussion on this), and there is an emerging trend of CSE services drawing upon neuroscience. There is a good deal of knowledge within this field that can help practitioners understand adolescent development (although some critics warn against making social policy claims prematurely on the available evidence – see for example Wastell and White, 2012). It is important, however, to be critically minded in the application of neuroscience and to avoid reductionist interpretations that ignore powerful influencing factors such as sex, ethnicity and poverty; it is also vital to challenge interpretations that might lead to a young person being considered irreparably damaged at a young age and being ‘written off’. In fact, the adolescent brain goes through a rapid process of development, and this process is fundamentally shaped by social interactions and relationships – thus this life stage offers a window of opportunity and should not be seen as a passing phase of immaturity to be tolerated whilst the child ‘becomes an adult’. This stage in itself is extremely valuable.
If considered critically, there are useful messages relating to adolescent brain development that can help practitioners translate presenting behaviours. For example, some researchers state that increased dopamine release to subcortical reward centres encourages attraction to new and immediately exciting experiences. This ‘sensation seeking’ behaviour is ‘strongly associated with the initiation of a wide range of adolescent risk behaviours such as use of drugs’ (Romer, 2010). This impulsivity may lead young people to engage in activities that present risk. Some argue that adolescents’ emotional responses are affected by a period of change in the limbic system of the brain, which governs emotional responses. ‘Teenagers may rely on their more primitive limbic system in interpreting emotions and reacting – “gut reactions”, since they lack the more mature cortex that can override the limbic response’ (Child Welfare Information Gateway, 2009). This, it is argued by some, makes them ‘more prone to engage in dangerous risk-taking behaviour’ and ‘not sufficiently able to interpret emotions, particularly if there is no secure attachment figure available to help them negotiate these tasks’ (Brown and Ward, 2013).
However, critics such as David Moshman (2011) argue there is no evidence for a significant difference in irrational behaviours, emotional maturity or ‘risk taking’ between adolescents and adults, with adults consistently being found to be as irrational and emotionally mature as adolescents. Moshman (2011) goes on to say that young children are distinct from adults in terms of neuroscience and neuropsychological development, but adolescents are not. Maturity, decision making, ‘risk taking’ and rationality tend to evolve in varied ways from the age of 10 or 11 onwards and many 14-year-old children function beyond the level of many 40-year-old adults. Whilst research often ascribes impulsivity, irrational behaviour, poor decision making and ‘risky behaviours’ to young people, Moshman (2011) argues there are no differences in these cognitive functions between adolescents and adults.
As noted here, evidence from neuroscience and neuropsychology is not uncontested. It is most useful to think about how brain development and social/environmental factors interact. And, to avoid placing responsibility with the young person, it is important to remain grounded in the firm principle that CSE is caused by child sex offenders, not children’s behaviours or experiences, and that all young people facing harm have a right to support and protective intervention under Sections 17 or 47 of the Children Act 1989.
As discussed in Section 2, there is often a lack of understanding of adolescent development with risk of harm being downplayed where practitioners perceive young people to be exercising ‘choice’; conversely, proportionate and non-excessive ‘risks’ are not always understood as being a part of normal adolescent development. Thus, the real vulnerability and risks that young people might face are not always reflected in policy and practice with the following potential consequences:
- Opportunities to work as a team with the young person, and often their family, in combating risk are missed.
- Resources are channelled to the wrong places because of misunderstandings about the fundamental drivers and contexts of risk (e.g., risk is assumed to be within the adult world rather than the peer group – see Firmin, 2013).
- Harmful assumptions are made about adolescent ‘choice’, which obscure vulnerabilities.
- There is a failure to recognise (and therefore address) the challenges involved in preventing and reducing adolescent risk (e.g., the frequent barriers to engaging young people in interventions).
- There is an assumption that in order for harm to be occurring, there must be a set of underpinning vulnerabilities (such as previously experienced abuse, neglect or harm which has ‘predisposed’ the child to CSE).
Like most child protection concerns, CSE is not a stand-alone issue; there are a range of inter-related factors and complexities that may, it is often assumed, increase vulnerability and a young person’s ‘risk’ of experiencing CSE. Authors have stated that these may include other forms of sexual violence or abuse, domestic violence, trafficking, antisocial behaviour or involvement in gangs (where victims’ criminal behaviour can further obscure the abuse experienced – see OCC, 2012), and going missing from home or care (Beckett, 2011b). These factors do not operate in a neat linear fashion and currently there is little empirical evidence to suggest a relationship with CSE.
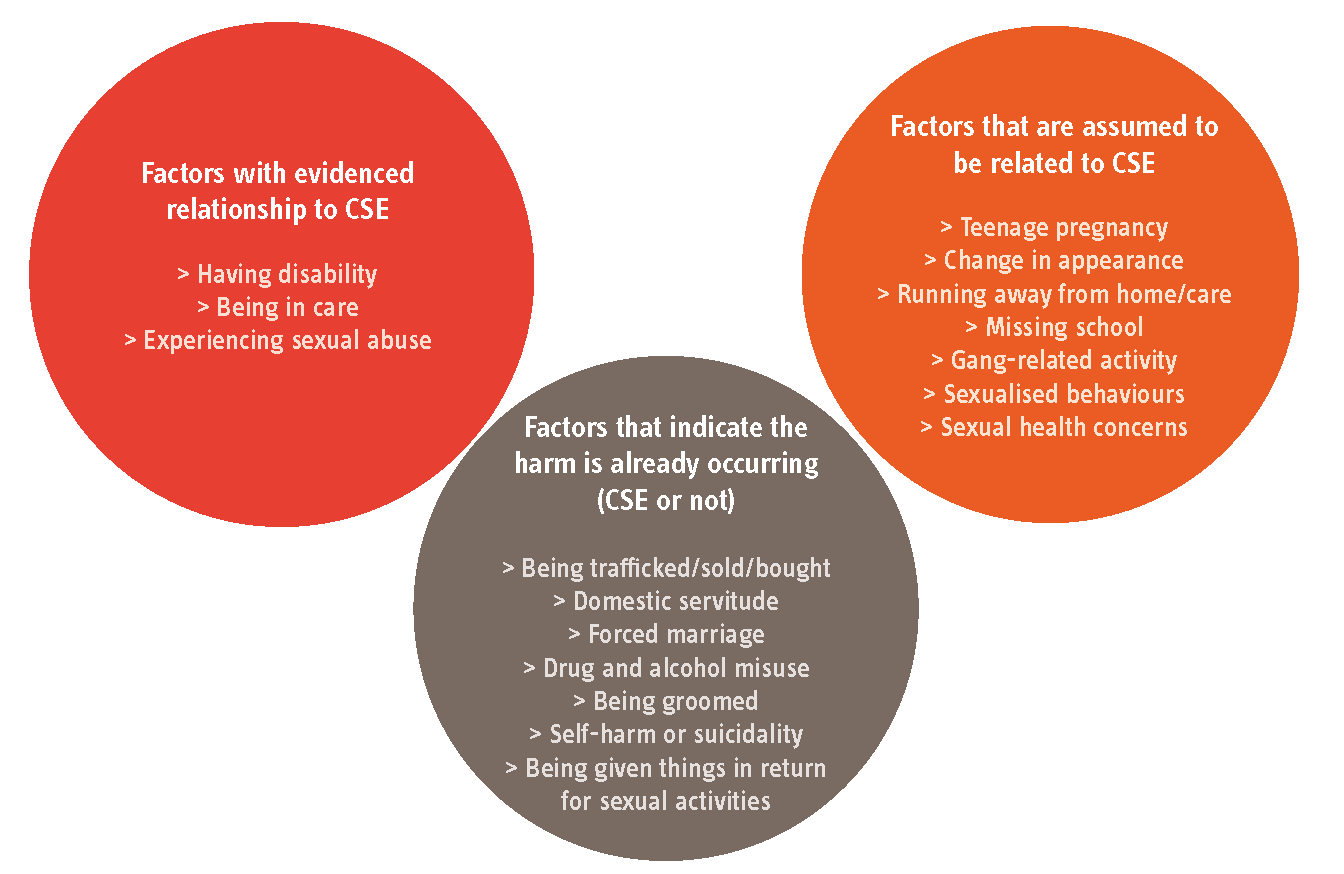
Figure 3.2: Factors contributing to vulnerability and risk of CSE
Figure 3.2 illustrates the current evidence in relation to ‘factors’ that are commonly thought to contribute to vulnerability to CSE. The first bubble contains those factors for which there is a strong evidence base in the literature (Brown et al, 2016; Gagne et al, 2005; Ullman and Vasquez, 2015). The third bubble contains examples of factors that are commonly referred to, but for which there is no robust evidence to show a causal or correlational link to CSE (Brown et al, 2016). The middle bubble shows factors that are commonly said to ‘contribute to vulnerability’ and are likely to be found in risk assessment toolkits and vulnerability lists for practice. However, they already describe significant harm to the child. It is arguably inappropriate to refer to such factors as ‘vulnerabilities’ or ‘risks’ because harm is already occurring to the child (and risk, commonly, is concerned with the potentiality of harm). This chimes with work by Brown et al (2017 forthcoming) that highlights the way that many CSE tools conflate risk and actual harm, in which indicators that are used to denote ‘low, medium and high risk’ are evidence of harm already occurring to the child and not an indicator of potential risk that has not yet occurred.
As more empirical research is conducted and the literature becomes more synthesised with existing literature on CSA, it is likely that this diagram and the associated evidence base will evolve.
It is vital to remember that not all victims of CSE have histories of adverse experiences, such as abuse, and not all children who are abused will go on to become victims of CSE. Similarly, it is important to remember that most children identified as having a number of ‘vulnerabilities’ will never experience sexual exploitation or abuse – and that vulnerabilities are not a prerequisite for a sex offender to target a child. When research and practice focus resources on searching for the vulnerability within the child that ‘contributed’ to CSE, this ignores the agency and strategies used by the sex offender to create opportunities to abuse and skillfully manipulate the child. Vulnerabilities are not the cause of CSE and removing or reducing ‘vulnerabilities’ must not be seen as the only solution to CSE.
This does not mean, however, that understanding vulnerabilities and adverse life experiences is not important. As Lalor and McElvaney (2010) note, victims of CSA are vulnerable to later sexual revictimisation; there is also a link between CSA and later engagement in high-risk sexual behaviour. Survivors of CSA are more likely to have multiple sexual partners, become pregnant as teenagers and experience sexual assault as adults. But all of these findings, including the high rate of revictimisation, are also
true for adult victims of sexual violence – so this is not unique to CSE or to children (Filipas and Ullman, 2006; Mason et al, 2008). Various models attempt to account for the inter-relationship between the resulting mediating variables such as isolation, withdrawal from education, low self-esteem, depression, anxiety, drug/alcohol use, post-traumatic stress disorder (PTSD) and distorted sexual development (Hanson, 2016; Allnock, 2016; Lalor and McElvaney, 2010; SBNI, 2014; Chase and Statham, 2005).
Understanding how different factors interact to increase vulnerability is particularly relevant in relation to children and young people who go missing from home or care, both because being ‘missing’ increases vulnerability and because running away can be a response to a young person feeling at risk where they live. However, the behaviour itself can become the focus rather than the cause, meaning that vulnerability is not addressed. In seeking to improve risk and vulnerability assessment, and respond to these messages from research, Wigan and Rochdale’s ACT Project 20 are trialling the use of a different pathway and strength based assessment tool which will be independently evaluated 21.
The interplay between CSE and going missing and gangs
While a range of factors may coexist and have potential links to CSE, evidence from the literature suggests two factors may be significant. In relation to CSE, ‘going missing’ (i.e., running away from home or care, being coerced to leave home, coming home late or being absent from school) and involvement (or interaction) with gangs are two significant factors that seem, for some children and young people, to interact with CSE (Coffey, 2014; Jay, 2014; Casey, 2015; Sturrock and Holmes, 2015). Coffey (2014) has identified that missing children are at risk of sexual exploitation and children may go missing because they are being sexually exploited. These factors rarely exist in isolation, however, and the young person is likely to be experiencing wider problems (Sturrock and Holmes, 2015). Even if they are not actually ‘missing’, children and young people operating without adequate adult supervision or boundaries is also considered a potential risk factor, especially when coupled with gang involvement.
This link between going missing and gang involvement is slowly gaining attention and beginning to have an impact on policy and practice, although gang-associated children and young people may still be criminalised rather than safeguarded (Sturrock and Holmes, 2015). As Sturrock and Holmes’ (2015) research for Catch22 Dawes Unit confirms, the needs and risks surrounding gang involvement are often not recognised in practice, in part because no national data is available to measure its prevalence. Yet the harmful effects on the children and young people involved are considerable. When children are involved in gangs or their lives are affected by gang activity, the response can become gendered. Girls are assessed and screened for CSE indicators, and boys are assessed and watched for violence and drug-taking behaviours. This ignores the wide range of abuses and harm children can experience regardless of their sex (Cockbain et al, 2015). This gendered approach is unhelpful because it results in a focus on the girls in a gang, an assumption they are being harmed via sexual exploitation, and a lack of focus on the boys in the gang. This ignores the many forms of criminal exploitation that can occur in gangs, which may have similar grooming techniques and perceived rewards or exchanges to CSE. Indeed, when approached for comment, many professionals from diverse specialisms agreed that the grooming techniques used in CSE, gangs, radicalisation and human trafficking are often strikingly similar (Hardy, 2016). There is also considerable debate surrounding the language that is used to describe children in ‘gangs’. Research by Medina et al (2013) found that peer groups of children are being labelled ‘gang members’ and discussed in terms of ‘gang association’ when in reality they are just in typical peer friendship groups. The same study argued that in discussions about children, there is evidence of confusion about ‘groups’, ‘gangs’ and ‘organised crime’ and an over-generalisation that children in groups must be in gangs.
Reflection pointers
- How are practitioners and frontline managers supported to develop their understanding of adolescent development and vulnerability?
- How do leaders challenge any potentially dangerous assumptions relating to vulnerable young people?
- How are our personal values (respectfully) explored in order to arrive at shared conceptualisations of ‘developmentally appropriate’ risk?
- In relation to CSE, how can we make sure practitioners are able to consider a child’s previous experiences without assuming that those experiences led to the CSE?
- How are practitioners defining and conceptualising ‘gangs’? How evidence-based are these conceptualisations?
- Do we have enough accurate and sufficiently detailed information relating to the issues of missing children and young people and gang activity to provide effective support to the children involved?
- And are we getting the information quickly enough? If not, what steps can we put in place to improve our local data collection and ensure it exerts a timely influence on local policy and practice?
- How can we make sure that services work in partnership so that safeguarding is prioritised alongside a criminal justice response?
- What strategies are we putting in place to ensure that those practitioners who work with young people in gangs (e.g., youth workers) are not working in isolation and that practitioners do not work in their own ‘silos’?
Key messages:
- Vulnerabilities and risks do not manifest in a neat linear fashion. They interact in complex ways that can both increase and obscure vulnerability.
- Practitioners need to be alert to the possibility of earlier trauma, but must avoid making assumptions about pathways to CSE.
- Practitioners must understand that the sex offender is responsible for the exploitation and harm of the child – adverse childhood experiences, ‘vulnerabilities’ or ‘risks’ alone are not enough to lead to CSE.
- Without timely and appropriate interventions, young people might be left to experience harmful risks and then blamed or held responsible for the outcome, as opposed to being seen as in need of support (Hanson and Holmes, 2014; Van Leijenhorst et al, 2010). Tackling this issue requires a sophisticated understanding of vulnerability, and of youth itself.
- Going missing and gang involvement are two risk factors that can, for some young people, interact with risk of CSE. The correlates of the relationship between the two factors and CSE must be acknowledged in practice, service design and local strategic responses.
Various authors and organisations have tried to set out the complex relationship between ‘risks’ and ‘vulnerabilities’ and how these interact with indicators of CSE. Table 3.1 attempts to show the breadth of factors potentially at play for young people set against an illustration of how child protection concerns may manifest in adolescence. It draws on work by Barnardo’s (2007a) in their Sexual Exploitation Risk Assessment Framework and the work of the Local Government Association (2014). It does not imply causality, nor does it imply that all of these factors will be present; and neither risk factors nor indicators are an exhaustive list.
As the later section on risk assessment makes clear, caution is needed when considering these potential indicators.
Table 3.1: Possible vulnerabilities in young people at risk of CSE (drawing on Barnardo’s, 2007a; LGA, 2014; Hanson and Holmes, 2014) (NB the above is not an exhaustive list nor are the factors listed in any priority of vulnerability or risk)
|
|
Child protection category and accordant manifestations of the risks that young people may face |
Vulnerabilities that may increase the risk of CSE (requiring further research)** |
Signs that young person may be being sexually exploited |
|
Sexual abuse * |
Sexual exploitation by gangs or groups Sexual abuse by peers Duress/coercion to sexually exploit/abuse others Online sexual abuse Intra-familial sexual abuse Sexual abuse by those in positions of trust or authority |
Attending school with children and young people who are already sexually exploited Disengagement from education * Disorganised attachment patterns associated with previous maltreatment Friends with young people who are sexually exploited Previous experiences of sexual abuse and negative experiences of sex Gang involvement or association Homelessness, including living in hostel, bed and breakfast or other unsuitable accommodation Instability and insecure relationships with families Learning disability Living in a chaotic or dysfunctional household with a disrupted family life * (may include parental substance use, domestic abuse/violence, parental mental health issues, parental criminality) Living in a gang neighbourhood Living in residential care Low self-esteem or self-confidence Previous exploitive relationships * Other gender-based abuse, risk of forced marriage, risk of ‘honour-based’ violence, female genital mutilation Recent bereavement or loss Self-harm, suicide attempts, eating disorders Substance misuse (drug or alcohol) * Young carer Poor health and wellbeing * History of disadvantage (child in need as opposed to child protection interventions) * |
Missing from home or care Physical injuries Drug or alcohol misuse * Repeat sexually-transmitted infections, and/or pregnancy and terminations Unexplained absences from school Change in physical appearance Evidence of sexual bullying and/or vulnerability through the internet and/or social networking sites Estranged from their family Receipt of gifts from unknown sources Recruiting others into exploitative situations Poor mental health Self-harm Thoughts of or attempts at suicide Exploitative relationships * |
|
Physical abuse * |
Family violence – adult(s) to young person Mutual family violence between adult(s) and young person Gang-related and community violence Physical violence from relationship partner |
|
|
|
Neglect * |
Neglect from family members, including rejection and abandonment (e.g., coercion to leave home) Parental mental health or substance misuse problems that disrupt parenting capacity and incur caring responsibilities on part of the young person Overly restrictive parenting Lack of developmentally appropriate boundaries and supervision Neglect in custody |
|
|
|
Emotional abuse * |
Emotional abuse from family members towards young person Emotional abuse between family members and young person Extensive bullying by peers and/or online Living with domestic abuse between parents Emotional abuse from relationship partner Problematic caregiving Exposure to other forms of abuse and maltreatment listed above |
|
|
* Denotes specific risk factors as identified in the Barnardo’s (2007a) Sexual Exploitation Risk Assessment Framework.
** As noted earlier, there is relatively little empirical evidence to support the large majority of these risk factors. Brown et al (2016) conducted the most recent and sophisticated review of all risk factors and indicators for CSE; out of 110 indicators, they found suitable evidence only for two – having a disability and being in care (previous sexual abuse was also noted, as discussed above). It is advisable to remain cautious about any risk factors, vulnerabilities or adverse experiences that are being linked to CSE without any empirical evidence and to keep up to date with the research as the topic matures and as the data is subjected to further scrutiny.
Hidden risks
It is important to acknowledge that both victims and perpetrators of CSE are diverse (Department for Education, 2012; Beckett et al, 2017) and hard to identify and, crucially, that some risks are not explicit (Hallett, 2015). Hallett’s (2015) qualitative studies with young people having experienced CSE revealed a key issue – that children often felt invisible to responsible adults who should have helped them, such as family or practitioners. Young people also conceptualised risks in their own terms. Engaging in behaviour that is typically described as ‘risky’ was presented by some as a means of coping with their own vulnerability – for example, ‘hanging out’ in crowds or ‘hiding away’ from face-to-face interactions to hide feelings. Some young people saw these behaviours as a means of taking back control, or facilitating basic needs such as money and housing (Taylor-Browne, 2002), which further highlights the complex nature of ‘choice’ and perceived consent in CSE.
There are also children who are unlikely to be identified as victims or ‘at risk’ of CSE because they do not show the stereotypical vulnerabilities and risks used in risk assessment toolkits. Children who are generally settled and have no vulnerabilities (as currently defined) and who are solely exploited online by sex offenders who have no intention of isolating them from family, changing their behaviours or asking them to meet in person, will rarely hit any of the criteria for intervention or identification (Palmer, 2015). Similarly, many risk indicators are female-centric, which is likely to reflect the under-identification of male victims at the point when many of these risk assessment frameworks were developed. Reliance on these toolkits and frameworks may in turn contribute to the significantly lower identification rate of boys who are sexually exploited – and who are instead often perceived either as gang members or perpetrators, even when displaying all of the same risk indicators as girls (Cockbain et al, 2015). There are also issues in relation to younger children, who can be sexually exploited but without the social freedom associated with the presence of indicators such as getting in cars, going to parties, meeting new people and drinking alcohol. Finally, as has been noted in relation to risk assessment in child protection more generally, there may be particular challenges surrounding the use of standardised risk assessment tools with children from BAME communities (Schrader-McMillan and Barlow, 2017; Turney et al, 2011). In relation to CSE, the indicators and vulnerabilities presented in assessment tools may miss the nuances, cultural differences and practices for children who live within what appear to be more ‘conservative’ communities, where there is an assumption that the families and wider community would know if a child was being sexually exploited (Fox, 2016).
For these reasons and others, there will be many children who are never identified due to the way risk and vulnerability are currently being understood in practice. Finally, it bears repeating that (a) not all children who are sexually exploited have any ‘risk factors’ or ‘vulnerabilities’, and (b) not all children who experience ‘vulnerabilities’ or ‘risk factors’ are targeted and sexually exploited.
.’Models’ of CSE and methods used
As professionals became more aware of CSE, it became increasingly apparent that the exploitation and abuse of children can take many forms. Over time various ‘models’ were introduced into practice and literature – however, we now understand that these ‘models’ are not underpinned by a robust evidence base and often do not draw on existing evidence-based models of child sex offending and grooming.
To categorise these forms of abuse in order to support practitioners to identify CSE, Barnardo’s (2011a: 6) introduced the concept of ‘models of CSE’ and described three core models:
- Inappropriate relationships: This usually involves offender who has inappropriate physical, financial or emotional control over a young person. There may be a significant age gap and the young person may believe they are in a loving relationship.
- The 'boyfriend' model of exploitation and peer exploitation: The perpetrator befriends and grooms a young person into a ‘relationship’ and then coerces or forces them to have sex with friends or associates. Again, the ‘boyfriend’ may be significantly older than the victim but not always.
- Organised or networked sexual exploitation or trafficking: Young people are ‘bought and sold’ or passed through networks where they may be forced or coerced into sexual activity with multiple perpetrators, as well as forced to recruit other young people.
In its online guidance the College of Policing 22 added the following models:
- Peer-on-peer exploitation: This refers to situations where young people are forced or coerced into sexual activity by peers or associates. This can sometimes be within gang activity, but not always.
- Gang-associated: A child or young person can be sexually exploited within a gang context, but this is not necessarily the common purpose of the gang. Types of exploitation may include using sex as a weapon between rival gangs, as a form of punishment to fellow gang members, and/or a means of gaining status within the hierarchy of the gang.
Whilst these models offered parameters for professionals and were likely to be helpful in raising awareness of different types of CSE, their deceptively simple descriptions can lead to confusion and controversy. First, all forms of abuse and exploitation could fit under the ‘inappropriate relationship model’; second, calling a model of CSE ‘boyfriend model’ does not adequately reflect the exploitation of boys and young men identifying as heterosexual and on the children who are exploited by a same sex perpetrator.
The 'boyfriend model' is hetero-normative and assumes a male perpetrator. The model also assumes a large age gap. Arguably, this model inadvertently perpetuates the stereotype of a young female victim with an older male sex offender and may exacerbate low identification rates of female child sex offenders and male victims.
A further problem is that these different manifestations can overlap – for example, peer-perpetrated CSE may equally be interpreted as fitting the ‘inappropriate relationships’ model or the ‘boyfriend model’, may or may not be gang-associated, and gang-associated CSE may or may not be linked to organised/networked exploitation and abuse. Finally, there is the argument that a child could easily ‘fit’ into all of those models at once, rendering them redundant as individual models. In reality, there are many scenarios that would constitute CSE under the current definition – many of which do not align with these models (Beckett et al, 2017)
These overlaps and oversights can create confusion and may lead to blind spots in practice if a child’s experiences of exploitation do not fit neatly into one of the models. A further point to make about ‘methods’ and ‘models’ of CSE is that there is some confusion between the two words (see following page for further discussion and explanation of ‘methods’).
It is important to remember that theories of sex offending, grooming and typologies of child sex offenders have been thoroughly researched, reviewed and tested in the forensic psychological and criminological literature and in practice since the 1970s and 1980s. They have also been theorised and discussed since at least 1892 (Marshall and Marshall, 2016; Boer, 2016). Therefore, there is already a substantial body of knowledge and evidence about the way sex offenders abuse and exploit children (alone and in groups), how they achieve their aims to harm children and how they perceive their offending. The ‘models of CSE’ do not represent models or theories of sexual offending against children and are better described as ‘examples of CSE’ or ‘manifestations of sexual abuse’. The literature and practice in CSE would benefit greatly from learning from the body of sex offender research from other fields of expertise.
What we do know about child sex offenders is that they have an extensive range of methods and approaches to grooming children for sexual abuse (Finkelhor, 1984) and sex offenders take many different pathways to abusing the child (Ward and Beech, 2006). In its online guidance the College of Policing 23 identifies the following methods that can be used to coerce a child (with the caveat that the list is not exhaustive – not all methods listed will be used, nor will they occur in the listed order):
- Giving presents – especially in the grooming phase
- Offering food treats
- Giving rewards such as mobile phone top-ups
- Giving the child or young person attention
- Offering false promises of love and/or affection
- Offering false promises of opportunities – e.g., modelling, photography, acting
- Supplying alcohol
- Drugs – either supplying drugs to facilitate exploitation, and/or young person being sexually exploited as a means of paying off drug debt
- Constructing situations whereby a young person must pay off debt
- Mental manipulation
- Blackmail
- Fear
- Physical violence.
The independent report by Ann Coffey MP (2014) found there was, among groups of young people surveyed, evidence of young men ‘disciplining’ their girlfriends through controlling behaviour such as constant phone calls, requesting proof of whereabouts and telling girls what to wear and say. In a review of Cafcass submissions to serious case reviews, Green et al (2014) found a ‘striking ambiguity’ around the status of the men involved in CSE, with many young people framing them as ‘boyfriends’. This fits with the grooming techniques used by sex offenders to manipulate or coerce young people into trusting them and build relationships over periods of time (which is common in other forms of CSA also).
Work undertaken into profiling the characteristics of perpetrators of CSE has found that most are male and their ages can range from school-age to elderly. This is not specific to CSE, however; it reflects the evidence base for sex offender characteristics for all types of sexual violence against adults and children. Whether they offend online or offline, against children or adults, the majority of sex offenders in the UK are male (Ministry of Justice et al, 2013). There is also the issue that young people who experience CSE can become involved with recruitment (OCC, 2012), with victims being groomed and coerced into recruiting and coercing other victims into CSE 24.When children who are being victimised by sex offenders are then groomed to recruit and exploit other children, it is important to remember they are still victims of exploitation – it is just the goal of their exploitation that has changed. The Children’s Commissioner’s Inquiry found that in relation to gang-associated CSE, perpetrators ranged in age from 12 to 75 (OCC, 2012: 102). Research by Barnardo’s (2013) also suggests that methods of exploitation are becoming more sophisticated, including the use of ‘parties’ to create networks for abuse, the use of technology to organise both online and offline abuse, and ‘internal domestic trafficking’ whereby children and young people ‘are moved from one place to another to be sexually exploited’. These methods have been confused in practice and literature as additional ‘models’ of CSE; however, it is important to recognise they are not models or constructs, they are methods to abuse and groom children for a sexual offence.
Reflection pointers
- How can we be confident that practitioners across services understand that CSE does not fit a particular model?
- What is in place to support practitioners (across services) and parents, carers and young people themselves to recognise the different methods employed by perpetrators?
- How effectively do our training activity and our recording processes reflect the understanding of how CSE manifests in our area? Or are outdated terms being used in these aspects of work?
Key messages
- There are a number of different ‘models of CSE’ which have been developed as the field has learned to respond to different cases.
- Models are problematic because they have a weak evidence base, they often overlap and interact – and some models can obscure vulnerability by being misinterpreted.
- Models can use unhelpful and stereotypical language and make assumptions that can affect practice and contribute to the development of blind spots.
- Understanding how CSE is manifesting locally is crucial for the development of an effective practice and service response.
- A variety of methods may be employed to groom a child for sexual exploitation and abuse.
- The existing evidence base for child sex offender models is extensive. This should be consulted and considered to learn about the methodology and typology of child sex offenders.
Grooming is not a linear process
Grooming is understood as the process which turns a sex offender’s fantasy into a reality (Whittle et al, 2013). Craven et al (2006) proposed the following definition:
As discussed above, CSE practice has not utilised effectively the empirical evidence available on the subject of grooming. This has led, in part, to oversimplification and the overuse of linear models of grooming, such as ‘the grooming line’ (Barnardo’s, 2007b; 2017: 14- 15), which can assume that grooming follows a linear model of:
- Targeting stage
- Friendship forming stage
- Loving relationship stage
- Abusive relationship stage.
However, there are many examples of CSE that do not include a friendship forming stage or a loving relationship stage. An example of this would be a child who is quickly threatened with violence or further harm if they do not perform sex acts for someone; or a child being sent a link to abusive imagery and then being blackmailed with being reported to the police if they do not take pictures of themselves and send them to a sex offender. Moreover, grooming is rarely linear (Whittle et al, 2013) and the methods offenders follow vary considerably. Sex offenders in CSE are not a homogenous group. They vary in the time they take to groom children and in their tactics, manipulation, charm, threat, intensity and general style, which tends to reflect the personality and goals of the sex offender, not the vulnerabilities or life of the child (European Online Grooming Project, 2012).
It is therefore vital that practitioners understand that grooming is not a linear, systematic process carried out by a homogenous group of sex offenders. Practitioners also need to appreciate that harm of the child does not occur only at the ‘end’ of a grooming process. Grooming is itself an offence and a source of harm and manipulation of the child. Linear models such as the grooming line imply that the harm only occurs at the end of the process which ignores the fact that the targeting, friendship forming and loving relationship (if those stages even occur) may also be harmful to the child. Finally, when applied to online offences against children, notions of linear grooming tend to identify harm with ‘successful’ physical contact with the child; in other words, practitioners assume that the sex offender has a goal to meet the child for a contact. In fact, many sex offenders have no motivation or interest in meeting the child to abuse them physically, because the online environment provides ample opportunity to abuse them without escalating the risk to themselves by meeting a child in ‘real life’ (Beech et al, 2008).
4. Recognition and assessment
This section is concerned with recognition of CSE. It explores disclosure and indicators and provides an overview of assessment practices and tools. Whilst it was not the remit of this work to undertake a scientific evaluation of the different assessment tools or frameworks, this section reviews the available assessment tools that appear to relate to research evidence by reflecting the correlates and context of CSE. An overview of the different assessment tools available and their characteristics as evidenced within the literature are provided in Table 4.1 at the end of this section. It is proposed that complexity theory may offer a useful theoretical perspective to underpin approaches to assessment, which has implications for service design and for supervisory practice (see Section 8 on workforce considerations).
Recognition of CSE
All practitioners working with young people have a safeguarding remit (HM Government, 2015a). This includes those working within education, policing, youth justice, youth work, community work, general practice, sexual health and third sector organisations, as well as social work – and others may well be involved also. However, research identifies concerns about a lack of awareness of CSE among practitioners and it is suggested this is a key reason for its under-identification (Clutton and Coles, 2008; Pearce, 2009a, 2014; Barnardo’s, 2011a). As Hallett (2013) notes, professionals who are non-specialists may not always refer because their awareness of the issue is low (see also Jago et al, 2011; Melrose, 2013). Furthermore, the context that makes a young person at risk of CSE, and the way practitioners make sense of a young person’s risk-taking behaviour, is influenced by their understandings about what CSE is (Hallett, 2013). In 2016, social workers were asked about their sense of competency and mastery when responding to concerns about CSA versus CSE. Despite CSE being defined as a form of CSA, the findings showed that social workers were not as confident in responding to CSE and felt that their skills were not transferrable from one form of abuse to another (Khwali et al, 2016). This lends support to those who challenge the usefulness of creating separate definitions (see Section 2.1)
As touched upon in previous sections, it is worth drawing attention to the fact that subjective interpretations of young people’s ‘risk’ can mean CSE may be missed because the young person is perceived to be troublesome rather than in trouble; or they may be perceived as making lifestyle choices and so less deserving of support (Phoenix, 2002; O’Connell Davidson, 2005; Pearce, 2009b; Beckett et al, 2017).
Reflection pointers
- How can we empower and support professionals across the system to recognise CSE?
- Are we doing enough to explore the different values and perspectives that may be held by different professional groups and their impact on identification and response?
Disclosure
While there are too many examples of young people disclosing CSE and not having their voices heard, it is also true that young people may not disclose what is happening to them – and boys in particular are less likely to feel able to disclose (Smeaton, 2013a).
There are a number of reasons which may explain why some young people do not disclose:
- Many young people do not realise the abusive nature of what is happening and therefore feel they have nothing to disclose (Beckett et al, 2017).
- They may feel in some way complicit in the abuse because there has been some kind of ‘reward’ or receipt of something (Beckett, 2011b).
- The young person may have engaged in an illegal activity, such as drug taking, and fear being criminalised on disclosure (Bedford, 2015; OCC, 2012).
- The young person may be afraid of not being believed or being blamed (Allnock and Miller, 2013).
The final report of the OCC’s Inquiry into CSE in gangs and groups identified that education to improve recognition, and services that facilitate the development of positive relationships and trust, make disclosure more likely (OCC, 2013a). It may be the case that investing in accessible visual media will help raise awareness and encourage children and young people to disclose and, potentially, even avoid exploitation (where this has not yet taken place); however, far more research is needed to understand whether and how educative interventions are effective.
In terms of facilitating disclosure, it must be acknowledged that children will not all follow the same trajectory to disclose CSE or ‘come forward’ to particular professionals even when encouraged. Smeaton (2014) evaluated The Children’s Society’s SELF Project (Sexual Exploitation, Live Freely), which was designed to raise awareness of CSE and provide support to victims and their families. The project ran a drop-in centre for young people to self-refer and receive support services, but take up was very low. Professionals involved with the project explained that young people may not always be in a position to recognise and confirm their own exploitation. Smeaton therefore stresses the need for professionals to ‘go out to’ young people. This emphasises the importance of close multi-agency working and community engagement to ensure there is a network of facilities for timely disclosure. Disclosure of abuse is complicated and contextual. Even when a child knows they are being seriously harmed and abused, disclosure is still unlikely; London et al (2005) found that 73 per cent of CSA victims delayed disclosure for at least a year and 45 per cent delayed disclosure for more than five years. Studies have searched for correlations between disclosure and age, severity of abuse, type of sexual abuse, relationship to the sex offender and other factors, but findings are inconsistent for all factors (London et al, 2005). The reasons for delayed or inhibited disclosure are varied, but van Loon and Kralik (2005a) found they included shame and embarrassment, fear of retaliation from the perpetrator, and concern about not being believed. This led to many victims discounting their experiences, denying they happened or choosing to block them out.
Naturally, there is a drive amongst professionals and the public to secure prosecutions and ensure that perpetrators are brought to justice – and prosecution is an important part of CSE being seen for the criminal offence it is. However, where prosecution relies on disclosure there are some important considerations. Describing abuse is traumatic and can re-traumatise victims of CSA – and repeatedly attempting to encourage a child to disclose abuse before they are ready can replicate the abusive dynamic (Harper et al, 2007). As Beckett and Warrington (2015) discuss, children who have experienced CSE can be encouraged or expected to disclose very painful experiences in order to support prosecution or investigation – which led the authors to conclude their report by questioning whose agenda is served by disclosure and prosecution, especially when it disempowers victims and removes choices. This issue is echoed by Ullman et al (2007) who found that having power over their disclosures and discussions about abuse reduces victims’ distress. Some survivors find disclosure helpful, others do not. If a survivor does not want to disclose, it might be because they are not ready, they feel it will re-traumatise them or it is not a necessary part of their ‘recovery’ (van Loon and Kralik, 2005b). In keeping with this message, Blue Knot released guidance for professionals working with sexual trauma that cited research showing that ‘ignoring the disclosure’ and ‘rushing them’ to disclose is experienced as particularly harmful by survivors of CSA (Blue Knot, 2017) 25. Barnardo’s recently published a report, ‘Journey to Justice’ 26 (Marsden, 2017), which highlights this issue further. The report explains that
Boys and disclosure
Boys are less likely to disclose experiences of exploitation and practitioners can find exploitation of boys harder to detect (DCSF, 2009; Barnardo’s, 2014a). Relatively few services specifically target boys. Analysis by Barnardo’s (2014a) of its CSE service users suggests that boys may be slightly younger at the point of referral than female service users, more likely to be referred by the criminal justice system and more likely to be disabled, with learning and behavioural disabilities the most common. Worryingly, Barnardo’s (2014a) research also suggested that professional attitudes were less protective towards boys, possibly because boys were more likely to express their trauma externally than girls and risked being assessed as ‘violent’ or ‘aggressive’. These findings were confirmed in 2015 by Cockbain et al’s (2015) quantitative analysis of individual-level data for 9,042 users of CSE services (one third of whom were boys). The analysis highlights the need for more research to understand why there are such different attitudes towards boys and young men who have been abused and what works for sexually exploited boys and young men in terms of service provision.
The BLAST Project provides specialist print and multimedia educational resources for boys and young men around CSE, as well as resources for professionals aimed at addressing discrepancies in professional assessments of risk in boys and girls. BLAST (Yorkshire MESMAC, 2015) worked with 20 existing CSE services and organisations to provide professional training and increase service accessibility to boys and young men. This work points to a need to improve the capacity of professionals to identify risks and make services more inclusive to boys while addressing boys’ potentially differing and specialist needs. After working in consultation with existing projects, the following suggestions were made (which could be widely applied in future service design):
- Publicity materials should feature boys as well as girls
- Appoint specialist workers to work with boys and young men
- Within CSE services, create an environment that is ‘less explicitly feminine’ to improve inclusivity.
An initial evaluation of the project found that partners had collectively increased their identification of boys and young men at risk of or experiencing CSE. Cross-cutting issues, such as partner engagement, were also an important factor in the project’s success (Yorkshire MESMAC, 2015).
Reflection pointers
- How confident are we that our CSE workforce is equipped to effectively identify and respond to boys experiencing CSE? Are we creating the right spaces for boys to facilitate disclosure?
- Is our literature and advice gendered in a way that might make it harder for male victims of CSE to disclose? What do boys tell us about how we support them?
- Are we equipped to deal with an increase in disclosures following increased awareness raising?
Indicators of CSE
There is a great deal of information available regarding so-called indicators of CSE (see Barnardo’s, 2015; HM Government, 2015c; Project Phoenix, 2014). This work served an important purpose at the point they were developed, but research now suggests a more nuanced approach is needed. For example, a framework aiming to help parents, professionals and young people ‘spot the signs’ of CSE 27 suggests that the key signs (which are also captured in Table 3.1) include:
- Going missing for periods of time or regularly returning home late
- Regularly missing school or not taking part in education
- Appearing with unexplained gifts or new possessions
- Associating with other young people involved in exploitation
- Having older boyfriends or girlfriends
- Suffering from sexually transmitted infections or becoming pregnant
- Unusual mood swings or changes in emotional wellbeing
- Drug and alcohol misuse
- Displaying inappropriate sexualised behaviour.
(Barnardo’s, 2015)
Despite these indicators being used widely across the UK in literature and practice, there are some important criticisms. As noted earlier (see Section 3.1), at present there is little evidence of any correlation or causation for the indicators currently being used in CSE (Brown et al, 2016). Authors of this work call for further and thorough research and urge caution in using these indicators to identify children affected by exploitation and abuse. It is suggested instead that they should be used as a non-prescriptive guide of potential things to look out for. The only two experiences that were shown to have a correlation (not causation, however) with CSE were being in care and having a disability (Brown et al, 2016); in addition, having previously experienced CSA is highly correlated with sexual revictimisation in the child sexual abuse literature (Gagne et al, 2005; Ullman and Vasquez, 2015). None of the other indicators, risks or vulnerabilities currently has any robust evidence to support a relationship or connection to CSE, and far more research is needed before they can be reliably used in any kind of predictive or standardised approach. Before any other indicators or screening tools are implemented, it is imperative that they are empirically tested on suitable samples to show reliability and validity (Brown et al, 2016).
Another justified criticism is that many of the indicators that practitioners and parents are warned to look out for are not indicators of potential risk, but evidence of harm already occurring. This is an issue because it means CSE is often being identified too late – long after early disruption of the sex offender or preventative work with children can achieve impact. When she spoke to children, Hallett (2017) found the young people she interviewed said early identification and prevention are the solution to the problem. If indicators are in fact only listing harm, they are not helping to identify CSE before it occurs; they are helping to identify CSE only when it has already begun.
Table 3.1 presents a very large body of symptoms, experiences, behaviours, actions, abuse types and difficulties that often appear in assessment and screening tools. They were evident in the sample used by Barnardo’s (2007a) at the time of developing the SERAF, but research since the time of development shows they do not demonstrate a correlation or causal link with CSE. That is not to say these issues don’t warrant attention, the indicators noted above (and in Table 3.1) all suggest potential difficulties or experiences that require attention and support.
Reflection pointers
- Are we confident that parents, carers and members of the community in our area are likely to know what the indicators of CSE are? Is there a risk that the tools provided to local professionals are not grounded in robust evidence?
- How can we be sure that practitioners across local agencies are fully aware of the complexities of relying on indicators of CSE, where these may lack evidence?
- Are we putting enough energy into supporting analytical skills and professional judgment?
4.2 Assessing needs and assessing risks
To support the identification and assessment of risk in CSE, it is common for assessments to explore the history, experiences and context of a child. History taking is important in assessment in relation to the young person’s experiences. Establishing a clear chronology, from the child’s perspective, can give crucial insight into the behaviours, coping mechanisms, experiences and perceptions of the child. Practitioners must not assume the young person has had a ‘difficult’ childhood; but nor should they assume that not being previously known to services means their childhood was without difficulty.
If practitioners rely only on linear risk assessment processes (this is discussed further below) or apply generic assessment without critical analysis, then they may lose the ‘individuality’ of that young person and fail to recognise their specific circumstances, realities and individual needs (O’Connell Davidson, 2005). By drawing on Brigid Daniel’s work around neglect (Daniel, 2010; Daniel et al, 2012), it is possible to conceive a simple framework that is focused on the young person’s individual circumstances. While recognising that there is a spectrum of vulnerability, and that increased vulnerability equates to increased needs, it may be useful when undertaking assessment for the practitioner to ask five very simple but significant questions:
- What does this young person need?
- What does this young person need me to think about?
- What does this young person need me to do?
- How will I know risks are reducing?
- What support do I need?
This will help to focus on both short and long-term needs as well as immediate safety issues.
These simple questions could be integrated into the five essential questions from the ‘See Me, Hear Me’ Framework (OCC, 2013a) and could be used at any stage in the assessment process, thereby helping to ensure that the young people are seen, heard, attended to and understood. Young people themselves articulate that protection and support can only be effective when these questions are answered.
Table 4.1: Asking and answering the questions that matter (Adapted from OCC, 2013a)
|
Questions from young people |
Questions for practitioners |
Practice messages |
|---|---|---|
|
Question 1 |
|
Don’t make assumptions about the young person and their needs. Don’t rely on what you are told – observe, interpret, check out, analyse – ask! Simply telling a child that they are being abused is rarely enough for them to fully accept or understand, and could induce trauma responses. |
|
Question 2 |
|
Establish (in partnership wherever possible) a clear plan to keep the young person safe and stop the abuse happening. Make sure the young person understands their plan and has had time and space to question it. Make sure the plan places a substantive focus on the sex offender, so that it doesn’t feel punitive or position the risk or responsibility within the child. |
|
Question 3 “Have you checked who else may be at risk?” |
|
Consider the safety of other children and young people, including bystanders and young people identified as perpetrators. Ensure that the child is not made to feel responsible for the safety of the other children or ‘used’ to gather information about other children. Also, ensure that other children and young people are considered as potential protective factors and not just ‘risks’. |
|
Question 4 |
|
Ensure that the support offered through the court process challenges any suggestion or implication of blame towards the young person. Make sure the child has access to full information about prosecution processes (created and written for their level of comprehension and language) well in advance of any court action and ensure they make choices about how they give evidence and how they are supported before, during and after. |
|
Question 5 |
|
Always respond positively; the child always has opportunities and hope for the future – that’s why you are working with them. Build their resilience and focus on strengths- based approaches It may take time for the child to feel that they have moved on. Recognise that the issues for this young person can re-emerge – and that this does not equate to failure on your part or theirs. |
It is vital that assessment practice is analytical in its approach and that critical thinking is applied when making sense of information. For information and training tools focused on this, see Research in Practice’s Handbook Analysis and Critical Thinking in Assessment (Research in Practice, 2014a) 28.
Reflection pointers
- Are we confident that professionals are aware of the factors that may increase a young person’s vulnerability to the strategies of those who seek to abuse them, including current factors around social context?
- How are practitioners supported to be analytical in their assessment of need? Are we doing enough to support them to be analytical? Are we doing anything that makes it more difficult for them to be analytical?
- Do assessment frameworks used locally facilitate an individualised assessment of the young person’s needs – including both those who are at risk of potential exploitation and those have already experienced harm?
Assessing risk
There is currently an important debate about whether CSE risk toolkits are valid and reliable, as explored above. Although risk assessment can only ever be largely indicative (rather than predictive), it is widely thought that if risk is assessed effectively, then alongside interventions to support or help the young person strategies can be put in place to remove the risk. Understanding and implementing accurate and ethical risk assessment and risk management is therefore essential to protecting children and young people from harm.
Macdonald et al (2014) point to the fact that risk assessment of vulnerable young people is not always consistent or thorough. Echoing the point above in terms of analysing need, they suggest that social workers can find it challenging to analyse complex evidence and reach an accurate judgement. They point to studies, such as Dorsey et al (2008), which suggest that some forms of risk assessment may only be marginally better than guesswork. Ofsted (2014) identified a lack of consistency in the completion of CSE risk assessments, as well as an absence of evidence to show that assessments were multi-agency in nature. According to Ofsted (2014), not only was the quality of risk assessment tools variable, but not all local authorities used a specific CSE screening or risk assessment tool to support multi-agency professionals in identifying early signs of CSE. It should be noted, however, that the use of screening tools is not without challenge. In Brown et al’s study on the use of tools and checklists to assess risk of CSE, it was suggested that some screening tools, particularly if completed by a professional / single agency without a full picture, can ‘screen out’ some young people where in fact they do require support (Brown et al, 2017 forthcoming).
A further examination by Ofsted of assessment quality (2015) found there had been broad improvements in how local authorities were carrying out their assessments in early help, children in need and child protection work. Although the report did not look at CSE specifically, some of the areas identified by Ofsted as needing further improvement do have significance in the context of assessing need and risk in relation to CSE:
- In most of the cases reviewed, social workers had carried out assessments as a stand-alone process, rarely updating written assessments when new information came to light.
- Social workers did not routinely share written assessments with families or children. When they did, the language used was often unclear and jargon was used.
- In a quarter of cases tracked, inspectors found that the assessment had not been timely enough, leaving too many children in circumstances where they were at potential risk of harm.
- 21 per cent of support plans did not clearly demonstrate the help that children and their families would receive and how the best interests of children would remain the greatest priority. (Ofsted, 2015)
These important findings by Ofsted (2015) illustrate some of the problems of assessing risk in practice. They are supported by further findings from Brown et al (2016), who found that many risk assessments used in CSE practice were neither reliable, valid nor tested to show effectiveness or accuracy. Brown et al went on to argue that indicators were largely evidence of harm already occurring to the child, and therefore do not assess or identify ‘risks’ in the true sense of the word (i.e., the chance that an unpleasant or harmful event may occur in the future). Overall, Brown et al (2016) concluded that the current approach to risk assessment in CSE has not been validated or rigorously tested and therefore should not be relied upon to make decisions about children. Instead, lists of indicators should be seen as a non-prescriptive guide of potential things to look out for and to discuss with colleagues.
CSE risk assessment tools are therefore not developed or tested enough to warrant scoring, rating or categorisation of children. As Brown et al (2017 forthcoming) note, the use of scored tools may be particularly problematic especially where narrative information is not possible to include, despite the fact that this narrative, qualitative information is vital in understanding and articulating indicators, risk and protective factors. Several local services are striving to innovate and improve alongside the evolving evidence base. For example, the Phoenix CSE risk measurement tool offers guidance notes which state “this is not a screening tool, nor is it meant to replace child and family assessments...this is a tool to assist a much broader social work assessment of the child’s strengths, needs and vulnerabilities”. The first version of the tool was developed in 2014 prior to the first Coffey report. It was updated and refreshed in 2016, drawing on the experiences of professionals across agencies in this process of updating. Several changes were made, including a greater emphasis on professional judgement, and social workers being explicitly encouraged to produce a chronology and capture the wishes and feelings of the child 29.
Reflection pointers
- How are practitioners supported to analyse risk, develop hypotheses and think critically?
- Do practitioners describe risk and needs in ways that young people and their families can easily understand?
- How do we know that practitioners adopt a partnership approach when undertaking assessments, in order to gain a full picture of risks and strengths?
- How will our service design facilitate a shift in the culture of assessment, away from reliance on prescriptive lists and towards an individualised analytical approach?
Key messages
- Victims of exploitation can come from any background and may have no prior ‘vulnerability’. While it is currently thought that apparent ‘vulnerability’ may increase the risk of exploitation, more research is needed in this area.
- The absence of vulnerability does not preclude young people being targeted.
- Assessing need in both the short and long term is important. Always, the focus must be on the individual needs of the young person.
- Good assessment requires analysis, a deep knowledge of the child and their life story, and critical thinking – it is not a list or a tick-box exercise.
- The young person’s voice must be central to assessment.
- It is important that the risk of CSE is acknowledged, documented and that agencies cross-reference information. Multi- agency screening tools that move towards a unified conceptualisation of risk are likely to be useful in supporting a shared understanding.
4.3 Approaches and tools
Local authorities use a range of approaches and tools to assess risk in relation to CSE. Barlow et al (2012) undertook a critical appraisal of available tools for assessing and analysing data about the likelihood of significant harm to children and report that, as yet, no universal method of assessment is established.
However, while there is arguably a dearth of research evidence around the effectiveness of specific risk assessment tools, particularly in relation to CSE, there are messages to be drawn around practice approaches and enabling systems. Barlow et al (2012) identified several distinct types of risk assessment tool that correspond to different stages of child safeguarding, in four broad categories:
- Risk assessment tools – these typically measure a limited number of historical and static factors to establish initial identification of need.
- Strengths and needs assessment tools – these measure dynamic factors, which may reduce harm if addressed.
- Response priority decision trees – these structured decision-making tools are used to improve and standardise decision making across professionals and facilitate the selection of appropriate responses to risks. These may be followed by permanency/ placement and reunification checklists, which are used to assess the likelihood of recurrence of harm in a given placement scenario.
- Audit tools – these are often used to audit whether cases have been classified accurately according to risk.
Barlow et al (2012) suggest that some ‘actuarial’ tools, including structured decision-making tools based on a decision tree approach, provided little in terms of descriptors of the domains being assessed – largely leaving interpretation to the practitioner. They advocate for baseline descriptors within a universal risk assessment framework for low, high and medium risk and standardised methods of assessing risk to aid professional judgment. Examples identified by Barlow et al (2012:22) include Safeguarding Assessment and Analysis Framework and Graded Care Profile (UK); Signs of Safety (Australia) and Child Abuse Risk Evaluation (the Netherlands).
While standardised tools have some limitations ‘they have the potential to improve the classification of risk of harm by providing practitioners with clear guidance about how to focus the assessment process, and analyse the data collected’ (Barlow et al, 2012: 22). This integrated approach to assessment aligns with emerging discourses on complexity (see Section 4.4) which highlight the nature of need as complex and question the appropriateness of using ‘predictive’ methods of risk assessment, endorsing the need for ‘indicative’ non-linear methods of assessing harm to children and young people (Barlow and Scott, 2010).
In applying the work of Barlow et al (2012) to the context of CSE assessment, we might deduce that risk assessment tools should:
- Be balanced – i.e., facilitate structured decision making without minimising complexity of individual cases or undermining professional confidence
- Be guided by a model of ‘working in partnership’ with children and families
- Be evidence based
- Provide ‘good guidance’ – i.e., use clearly defined and comprehensive behavioural descriptors to guide the assessment and categorisation of risk.
Specific assessment tools reviewed within this scope
As mentioned earlier, this scope does not evaluate the tools; rather it identifies a number of tools that reflect to some extent the messages from research and offers an overview of their components and characteristics.
- Phoenix CSE risk measurement tool: This tool developed via Project Phoenix (2014) attempts to consolidate a singular definition of CSE among stakeholders (social services, police, NHS and local community services as well as national charities) to foster improved multi-agency assessment and working across multiple local authorities. This is in line with Coffey’s (2014) recommendation of facilitating better cross-border working. The tool also provides a guided and cumulative scoring system for risk assessment, with overall scores relating to lower, medium and high risk levels, enabling a child to be assessed on a range of criteria. The tool aims to provide a universal means of assessing risk to improve understanding and streamline perceptions of risks across agencies. The critique offered by Brown et al (2016) (see earlier discussion) is relevant to this tool, however it should be noted that the tool was reviewed and revised in 2016 and that this has led to a number of useful changes. The tool now emphasises professional judgement and the child’s voice. In a connected piece of work, Wigan and Rochdale’s Project ACT has developed a new approach to screening and assessment, co-produced with young people, which allows children to have a voice in identifying needs and strengths and draws on the research evidence about risk and participation 30.
- The Safeguarding Assessment and Analysis Framework (SAFF) (Bentovim et al, 2010): A decision-making tool which addresses the three domains of the statutory guidance provided to professionals (‘the Assessment Framework’ – DH, DfEE and Home Office, 2000) – i.e., the young person’s development needs, family and environmental factors, and parenting capacity. It can be helpful as a decision-making tool that also factors in an assessment of future change.
- Graded Care Profile (Srivastava and Polnay, 1997): This strengths and needs based, objective assessment model was updated in 2015. GCP2 includes assessment in relation to four categories: physical care, safety, emotional (such as love between carer and child) and developmental (such as being encouraged to learn and being praised) 31. (For an evaluation of the earlier GCP, which informed development of GCP2, see Johnson and Cotmore, 2015.)
- The NWG (formerly The National Working Group Network on Tackling Child Sexual Exploitation) has provided a CSE risk assessment tool that allows practitioners to explore some of the vulnerabilities and indicators present in a child or young person who might be at risk of or experiencing sexual exploitation. It provides a framework to help practitioners think about the risk to the young person and about what to do with the information they have. A new tool is being launched by NWG in 2017 32. This new tool moves away from a scoring and tick box approach and is designed to be used to inform rather than determine professional judgements. NWG emphasise that this approach will require good engagement with children and their families to complete the assessment. At the point of publishing this revised scope, the new tool has not yet been rolled out for testing; the critique offered by Brown et al (2016) is relevant to this tool.
- Children Abused Through Sexual Exploitation Project (CATSE) (Lebloch and King 2006: 371) provides an example of a strategy for assessment that emphasises establishing levels of risk in CSE. It aims to address ‘[the] practitioner’s struggle with the blurred boundaries between adolescent sexual exploration and adult sexual activity’. This was overcome through frequent multi-agency training (which included managers) and establishing a risk framework with levels of risk believed to be associated with CSE (such as substance use, sexual and emotional health). The key message here is that training is required to ensure consistency, and it is helpful to provide descriptive examples to determine level of risk with each factor. As this tool uses indicators of CSE which currently have a weak causal or correlational evidence base, the critique offered by Brown et al (2016) is relevant here also.
- Brook Sexual Behaviours Traffic Light Tool: This tool aims to help children’s professionals categorise sexual behaviours in order to identify risk and safeguarding concerns.33 The tool is based on research into the harmful sexual behaviours of children. It provides detailed descriptors of sexual behaviours for different age groups and categorises them as green (safe and healthy behaviour appropriate for age), amber (potentially outside of healthy behaviours) or red (outside of healthy sexual behaviours). The tool does not include risk categories and relies on training and the understanding of the professional to identify CSE risks; it may be helpful in identifying indicators of peer-on-peer abuse. Brook also offers training courses for professionals in using the tool, which may be useful in exploring the way that the perception of sexual behaviours in children differs between individuals and cultures.
- ‘Spotting the Signs’: The British Association for Sexual Health and HIV (BASHH) Adolescent Special Interest Group and Brook developed a tool to help health professionals detect signs of CSE among young people attending services for sexual health (Rogstad and Johnston, 2014). The standardised pro forma, which can be used alongside existing sexual and social health frameworks, was launched in 2014 following a successful pilot in sexual health clinics, outreach settings and general practice. This tool is not an assessment framework for CSE, nor is it predictive or indicative. It is better described as an information-gathering, needs-based questionnaire about the whole life of the child, producing good feedback from the young people who helped to pilot it.
- Sexual Exploitation Risk Assessment Framework (SERAF): Developed by Barnardo’s for use in Wales as a screening tools for professionals. It includes a checklist of vulnerabilities and moderate/significant risks to produce a cumulative score that corresponds to different levels of risk (banded ‘no risk’, ‘mild’, ‘moderate’ and ‘significant’). In a pilot study (Clutton and Coles, 2008) practitioners reported that the tool proved useful in the identification of risk and could easily be incorporated into different working practices. However, the tool has not been rigorously tested, and the indicators are not currently supported by a strong causal or correlational evidence base; therefore the critique offered by Brown et al (2016) is relevant to this tool.
As noted above, Brown et al conducted an exploratory study of CSE screening and risk assessment tools (2017 forthcoming). Through interviews and surveys with practitioners across the country, authors report that CSE tools are being used with significant variance. Their findings raised concerns about the discriminatory nature of CSE toolkits, arising from the fact that they are not empirically tested, validated or evaluated. Authors note that many existing CSE tools are inappropriate for boys, younger children and disabled children – who may experience, present and respond differently to adolescent girls (on which the CSE toolkits are often based).
Brown et al. (forthcoming) also report that many tools do not focus on the strengths of the child, their families or their immediate environment – meaning that the toolkits represent a deficit model of working with children and young people where their experience of CSE is the sole focus. Rather than seeing the child as a whole person who became the victim of a serious crime committed by another person, the child is assessed and perceived as a problem to be solved; their strengths, potential, skills, personality, support and protective factors are ignored whilst ultimate focus is placed on their ‘risks’ and ‘vulnerabilities’. The strengths-based tool developed by Wigan and Rochdale’s Project ACT, and co-produced with young people, is an example of local services’ efforts to adapt and improve in line with the evolving evidence base.
Key messages
- Standardised tools should be used in tandem with professional judgement to assess the likelihood of harm. A non-linear approach ensures that complexity is not minimised (see Section 4.4).
- Screening tools without an evidence base or proof of validity/reliability should not be used to make decisions about children.
- Tools must recognise strengths and wider contextual factors, and must be used non-prescriptively to enhance professional judgment.
Reflection pointers
- How do we know our assessment tools are fit for purpose? How are we assured of the evidence base underpinning them? How do we assess the impact of these tools on practitioners’ knowledge, skills and confidence?
- How can we be sure that professional judgment is enhanced by, not undermined by, the tools provided to practitioners? How do young people and families affected by CSE experience the tools we use?
4.4 Considering complexity theory in relation to assessment
As mentioned above, Barlow and Scott (2010) endorse the need for ‘indicative’ (as opposed to ‘predictive’) non-linear methods of assessing harm to children and young people. Within CSE and child protection generally there is currently much focus on risk assessment; while it is of course essential to recognise risk, one criticism of this approach is that it presents a linear system. This section discusses how complexity theory could facilitate understanding of the issues practitioners face when working to address CSE effectively. Drawing on the work of Stevens and Cox (2008), it is suggested that complexity theory offers helpful ways to conceptualise and work with the processes that underpin keeping children and young people safe from the harm of CSE.
A lack of analysis and critical thinking has consistently been highlighted in a number of serious case reviews, inquiries into child deaths and inspection reports (Brandon et al, 2009; 2010; 2012; see also Ofsted’s 2015 report of its thematic inspection on the quality of social work assessments). Assessment practice in child protection has been criticised for adopting a procedural, checklist approach (Munro, 2011). The use of non-linear concepts to underpin assessment may be useful in helping practitioners to be more analytical in practice through deeper understanding of the context and complexity of CSE. If practitioners are supported to be more analytical in practice and in their assessments, this might help them critically analyse complex situations and recognise non-linear variables (Brown et al, 2014). It is important to consider organisation-wide approaches to assessment as practitioners cannot change practice without systemic support. Complexity theory provides a framework for understanding the processes involved but without the problems of reductionism (Stevens and Cox, 2008).
Complexity theory, which is mathematical in its origins, tackles the understanding of complex systems. It presents an alternative to linear systems theory approaches and has applications for social work practice. Safeguarding more generally, and specifically work to address CSE, is itself a complex system. It is suggested that reductive approaches to vulnerability assessments and interventions can limit practitioners’ ability to respond to and adapt to the variance and multiplicity of an individual’s needs (Stevens and Cox, 2008). Unlike ‘closed’ linear systems, complex systems are ‘open’, liable to be shaped by their environment (including in the case of CSE, by practitioners themselves) and prone to abrupt change. Young people operate in social groups made up of agents interacting with one another in multiple and contingent ways to form complex adaptive systems. Drawing upon the concept of self-organisation, it can be demonstrated that behaviour is as much a product of interactions between agents and their environment as it is a result of individual actions. One person’s behaviour affects others – but that person is in turn affected by the behaviour of the other and by their environment. It is in these interactions that the young person self-organises (Read, 2002) and the factors that lead to exploitation within a group can be conceptualised as a self-organising system. The recognition of this adaptive system and of the multi-faceted complexity of the young person’s experience can help practitioners to seek a different ontological position in assessing need and identifying possible outcomes when working with high-risk vulnerable young people.
Furthermore, on a practical level, whilst ‘actuarial’ risk-assessment tools are more precise when identifying the risk of harm (D’Andrade et al, 2008; D’Andrade et al, 2005; Stewart and Thompson, 2004) they may be inappropriate in situations where fast- paced professional decision making is required (Breckon and Hay, 2015; Coveney and Highfield, 1996). Complexity theory may help to give a better understanding of risk by allowing the practitioner to recognise that a young person’s needs, vulnerabilities and risks are dynamic and inter-related and to recognise that they, as the practitioner, are one of the variables in that young person’s life.
The need for non-linear understanding
A practitioner who tries to undertake risk assessment by simply noting or adding up the risk factors is applying linear understanding. In linear understanding, A plus B always equals C. Complexity theory suggests this is not an adequate way to deal with complex phenomena, such as assessing the risk for CSE. Complex adaptive systems are non-linear. Thus action A plus B may lead to C, but it may also lead to D, E and/or F (Stevens and Cox, 2008). Action may therefore lead to no change, or even a change for the worse. A non-linear approach helps to recognise that outcomes cannot necessarily be predicted, as there are different variables that might impact on the young person and how they respond to the potential or actual exploitation. Coveney and Highfield (1996) also suggest that complexity theory supports the development of indicative (rather than predictive) models of risk, which may also help to avoid labelling young people or blaming them for the choices they have made.
Stevens and Cox (2008) draw attention to the repeated finding that inter-professional communication and collaboration is often lacking. Reviewing the hundreds of recommendations around CSE indicates that the tendency has often been to increase linear responses (more protocols; more regulation) in the hope that this will eventually ‘leave no margin for error’. However, Stevens and Cox (2008) argue that the opposite appears to be true: children and young people continue to suffer mistreatment, abuse and exploitation and high-profile oversights in safeguarding continue to be exposed. Simply identifying the risk factors cannot predict when, how or why CSE will occur (Stevens and Hassett, 2007). Taking a linear approach may lead to a false sense of security and an assumption that outcomes can be predicted, whereas in reality minor changes can have a major impact in a complex system. Linear approaches can also lead to a ‘blame culture’ (Stevens and Cox 2008), wherein searching for causal factors means that the interplay of multiple complex factors are ignored. This blame can be directed towards young people (for not ‘making good choices’ for example) and towards practitioners (for ‘failing to keep young people safe’).
Systemic or systematic assessment
Complexity theory differs from systems theory, which has more traditionally been used in the context of practice, although there are linked ideas between the two. Systems theories have a long history in social work practice, dating back to work on general systems theory by writers such as Pincus and Minahan (1973), family systems (Minuchin, 1974) and in ecologically based ideas such as those of Bronfenbrenner (1979). However, Stevens and Cox (2008) argue that practitioners should make a distinction between systemic and systematic. Traditional systems models have operated from the stance that if a system is understood, then the system is knowable and the future can be predicted. In this sense, child protection processes are systematic; so while following procedures can put practitioners at ease, it can also lead to a false sense of security which might not be helpful when working with the bigger picture of CSE. And while existing models such as the Assessment Framework (DH, DfEE and Home Office, 2000) are ecological in their design, they tend to follow specific (systematic) processes.
In order to protect against applying such models in a way that might be reductionist or systematic, it can be helpful to use systemic techniques such as eco-mapping or ‘mind mapping’ based on scenario building with families, where young people actively contribute to the assessment. As Stevens and Cox (2008) point out, it is the narrative that provides the detail and allows complexity concepts to be put into action. Stevens and Cox (2008) argue that in order to facilitate this, access to reflective supervision – where practitioners recognise their position within the system and the impact on other variables – is essential; reflective supervision will help ensure the assessment of the young person is dynamic. (Supervision is discussed later in the scope in Section 8 on workforce considerations.)
Complexity theory may benefit local strategic activity too. Localised intelligence-led approaches (driven by multi-agency information sharing) can help to identify risk ‘hot spots’ or methods being used to exploit young people locally, thereby using geographical and systems angles (as well as the intra/inter-personal) to identify young people at risk . This mirrors the way eco-maps are used in social work or counselling to illustrate the ecological system that encompasses an individual and their family patterns, or the way mapping is used by police to detect serious organised crime networks. In the case of CSE, vital pieces of ‘soft’ intelligence may be held by family members, members of the community and professionals; these need to be gathered and consolidated to build an accurate picture of risk and so prevent or disrupt exploitation (Coffey, 2014; Project Phoenix, 2014.) This information can do more than highlight individual perpetrators and young people at risk; it can also help build a network of relationships and so enable more complex problem profiling (Project Phoenix, 2014) which can aid both police and social work.
Reflection pointers
- Is there a danger that our language, processes or assessment tools encourage an approach to assessment that is reductive, narrow or unrealistic?
- For practitioners, are we striking the right balance between providing evidence-based tools but also promoting reflective and non-linear analysis of risk?
- How might complexity theory add value to our assessment practice?
- How can we be sure that practitioners locally are undertaking assessments in a way that is genuinely systemic, rather than just systematic?
- Do local service leaders ‘role model’ an understanding of complexity theory and non-linear understanding of risk?
Key messages
- When children experience – or are at risk of – sexual exploitation, the relationship between their needs, their vulnerabilities, the harm being done to the child and the risk coming from the sex offender can create a dynamic and complex situation for the child and the practitioner.
- Taking a linear approach to understanding the young person’s experiences, harms and the risks presented by the sex offender can lead to over-simplification of assessment and interventions. It can create a false sense of security and an assumption that outcomes can be predicted; in fact, in so complex a system as the life of a child at risk of (or experiencing) CSE, minor changes can have a major impact.
- While 'actuarial' risk-assessment tools are more precise when identifying the risk of harm, they may be inappropriate in situations where fast-paced professional decision making is required. More research is needed before any definitive approach can be recommended.
- Considering complexity theory may facilitate a non-linear approach to assessment and intervention in CSE which could reduce victim blaming of children and families.
Table 4.2: Characteristics of various assessment tools
| Tool | Type of Risk assessment | Professional audience | Structured decision making | Detailed behavioural descriptors / guidance | Professional judgement / rating required | Assess YP’s short-term needs | Assesses YP’s ongoing needs | Assesses YP’s understanding | Assesses environment factors | Assesses parenting capacity | Assesses strengths |
|---|---|---|---|---|---|---|---|---|---|---|---|
| Phoenix CSE risk measurement tool Project Phoenix (2014, revised 2016) | CSE | Multiagency | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | No |
| Not a screening tool, nor is it meant to replace child and family assessments. Includes statement of wishes and feelings of young person. Tool can be used in subsequent assessments to compare progress. This tool requires further validation, evaluation and stronger evidence base for indicators. |
|||||||||||
| Safeguarding Children Assessment and Analysis Framework (SAAF) Macdonald et al (2014) | General | C &YP Services | Yes | Yes | Yes | Yes | Yes | Not clear | Yes | Yes | Yes |
| The model features steps for risk assessment and intervention. | |||||||||||
| Children Abused Through Sexual Exploitation Project procedure (CATSE) Lebloch & King 2006 | CSE | Multiagency | Yes | Yes | Yes | Yes | Yes | No | Some | No | No |
| The procedure includes a tool for establishing risk levels, but also features a framework for multi-agency approaches to CSE. This tool requires further validation, evaluation and stronger evidence base for indicators. | |||||||||||
| Brook Sexual Behaviours Traffic Light Tool Brook – adapted from Family Planning Queensland (2012) | CSE, CSA & HSB | Multiagency | Yes | Yes | Yes | Yes | No | No | No | No | No |
| Categorises risk behaviours by age group, based on literature and research evidence of harmful and developmentally normal sexual behaviours. Perceptions are affected by cultural and religious norms. | |||||||||||
| BASHH & Brook Child Sexual Exploitation (CSE) Pro forma ‘Spotting the Signs’ Rogstad & Johnston (2014) | CSE | Health | No | Yes | Yes | Yes | No | Yes | Yes | No | No |
| A questionnaire for healthcare practitioners to use in consultations with young people. This tool does not assess or mention CSE, or use any indicators. It is a whole-person approach to gathering information about the child and their life. | |||||||||||
| Sexual Exploitation Risk Assessment Framework (SERAF) Clutton & Coles (2008) | CSE | C &YP Services | Yes | Some | Yes | Yes | Yes | Yes | Yes | No | Yes |
| Includes level 1 and level 2 risk assessment pro forma. Includes element which assesses young person’s own understanding of their safety. This tool requires further validation, evaluation and stronger evidence base for indicators. | |||||||||||
| Recognising Child Sex Exploitation Tool National Working Group | CSE | Social work/ specialist CSE services | Unclear | Yes | Yes | Not clear | Not clear | Not clear | Not clear | Some | Unclear |
| This tool requires further validation, evaluation and stronger evidence base for indicators. | |||||||||||
| Graded Care Profile (GCP) (Srivastava & Polnay, 1997) | General | C &YP Services | Yes | Yes | Yes | Yes | No | No | Yes | Yes | Yes |
| To be completed with the child and their primary caregiver. A copy of the profile is provided to the caregiver. | |||||||||||
NB Table 4.2 is designed to provide a brief overview of the various CSE risk assessment tools available and to briefly indicate their particular functions. It is not an evaluation. Acknowledging that the tools featured are designed for differing domains of professional use does not provide a rating of their coverage.
5. Interventions
With no singular approach as to how local authorities organise multi-agency responses to CSE or clear guidelines currently available on the exact role of social workers in this process, it is perhaps not surprising that social workers express less confidence in dealing with CSE and online abuse than other types of abuse and neglect (Martin et al, 2014; Khwali et al, 2016). This section explores the evidence around CSE interventions across the spectrum of support. In the absence of a wide body of scientific research regarding discrete interventions, it seeks to draw out messages as to wider approaches and interventions which may be more effective.
5.1 Overarching messages regarding models for intervention
Some useful principles for an effective local response can be drawn from the ‘See Me, Hear Me’ Framework, which was developed following the Children’s Commissioner’s Inquiry into CSE in gangs and groups (OCC, 2013a: 54-89) and piloted from late 2014 by Brighton and Hove City Council, Oxfordshire County Council and Sandwell Metropolitan Borough Council. The two-year pilot was evaluated by the University of Sussex (Hickle et al, 2017). The framework identifies the essential things that need to be in place to ensure effective local responses to CSE. Its evidence base is drawn from the OCC’s two-year inquiry and its principles can be adopted and included in local CSE pathways and the development of new services:
- Each child or young person who is being sexually exploited has a comprehensive multi-agency assessment of their needs, after which meetings are held to consider the needs of the CSE victim and their family and to devise a plan to meet those needs.
- Support services are delivered to meet a child or young person’s needs on an individual basis, promote the development of an enduring and trusting relationship between the young person and supporting professional, and are based on a clear understanding that one size does not fit all.
- Support is provided to parents and carers separately from the support made available to the child or young person. Appropriate information on sources of support – for example, PACE (Parents Against Child Sexual Exploitation) 34 – is readily available to every parent and carer.
- Practitioners should be encouraged to ‘think family’. While interventions should be young person focused, family support may also be required and should be provided through family support workers.
- > Disruption of CSE and investigation is integral to every young person’s CSE plan.
- Safeguarding and disruption activity is not dependent on a direct disclosure from a young person.
The final evaluation report for the Barnardo’s Families and Communities Against Sexual Exploitation (FCASE) project (D’Arcy et al, 2015) also identifies some key messages for direct work with young people and their families. These include:
- Work with parents and carers alongside young people using a strengths-based approach
- Equip families with knowledge and information to help them safeguard their children
- Promote the role of the voluntary sector in building bridges between families and the statutory sector
- Engage workers who have specialist knowledge and relational skills
- Ensure continuity of workers to help build trust and productive relationships
- Provide effective training that makes appropriate and accurate referrals more likely. (D’Arcy et al, 2015: 25-26) Many of these themes and principles are discussed throughout the rest of this section.
Some argue that investing in specialist services may yield financial benefits. For example, Barnardo’s highlight the pivotal role of specialist interventions, not just in helping victims recover from CSE but also in minimising the costs associated with it. Based on an estimate of how young people’s level of risk changes in the absence of an intervention, Barnardo’s (2011b) research briefing Reducing the Risk, Cutting the Cost, produced with Pro Bono Economics, shows a potential saving of £12 for every £1 invested. The evaluation of the Wigan and Rochdale ACT pilot suggests cost benefit on accommodation costs; New Economy 35 calculated that for every £1 spent within the ACT project, £4.25 was saved (Scott et al, 2017). Further research will enable greater understanding of cost benefits in future.
The NWG suggest CSE is more likely to be addressed effectively where there are dedicated CSE workers. Where there are dedicated services, the suggestion is that other professionals in the area are more likely to be aware of CSE, know how to identify it and know who to refer to (NWG, 2010). The opposing argument, however, is that the rise of specialist CSE workers since 2010 has led to some experienced social workers, who have been supporting children and families with CSA for many years, now experiencing reduced confidence and skill to support cases of CSE (for example, see Martin et al, 2014; Khwali et al, 2016).
It is not enough to commission services with specialist expertise. Attention must be paid to the over-arching model being embodied by services and practitioners. Fargion (2014) argues that child protection models are potentially restrictive and damaging, as they focus on negative correlates and neglect the strengths of a child or their family (an argument also made by Featherstone et al, 2014, and PACE, 2014). This can result in practitioners approaching cases with suspicion, which can create a distancing effect between young people, families and practitioners and a reluctance to disclose information. By contrast, Khoo et al (2002) compared social work interventions in child maltreatment in Sweden and Canada and found that social workers adopting a child welfare model were more likely to undertake early interventions and would decide to take action based on an individualised assessment of a child. Table 5.1 provides a comparative overview of the child welfare model and child protection model, alongside the advantages of a more welfare- orientated approach.
Table 5.1: Child Protection and Welfare Orientation (taken from Fargion, 2014)
|
Child Protection Model |
Child Welfare Model |
Child Welfare Model - Considerations for practice |
|---|---|---|
|
Best interests of the child are narrowly focused on protection |
Best interests of the child are broadly defined to include the welfare of the family |
Supports the ‘Think Family Model’ |
|
Law-led rather than discretion-based |
Discretion-based |
Individual needs are more likely to be identified and therefore need to be addressed |
|
Assessment is based on tools (which may or may not be standardised or evidence-based) |
Assessment is based on interaction between family and social workers |
Allows for professional judgement but can work in conjunction with a standardised tool |
|
Aims for objectivity |
Acknowledges different perspectives |
Enables realism |
|
Centred on difficulties and problems |
Considers difficulties as well as strengths and resources |
More holistic |
|
Treats difficulties as signals of risk |
Seeks to understand difficulties in order to find ways to provide support (and early help) |
Should enable the reality to be visible rather than occluded by myths |
|
Restricts professionals’ discretionary powers |
Enhances professional strength |
Empowers practitioners, requires other means of ensuring consistency |
|
Less readiness to intervene, though intervention may arguably be experienced as intrusive when it happens |
More readiness to intervene, though arguably intervention may be experienced as less intrusive |
Upholds the rights of children and young people to be protected from exploitation and the resulting harm |
|
Individual rather than community- oriented |
Community-oriented |
Facilitates an integrated approach, though communities will vary |
|
Remedial rather than preventive |
Preventive rather than remedial (facilitating long-term solutions) |
Promotes resilience in the children and young people |
Lastly, the urgency with which local authorities seek to address the needs of high-risk young people experiencing CSE must not lead them to overlook the critical importance of prevention and early intervention.
Reflection pointers
- How would young people and families describe our approach?
- Are we adopting a child welfare approach or a child protection approach? Can we explain why?
- Are we striking the right balance between ensuring effective services for high-risk young people, and investing also in effective prevention and early help approaches?
- If we are investing in specialist CSE workers, how are we capturing the impact of this (including any unintended negative impacts)? How are we ensuring that any cost benefits of CSE services are being accurately captured?
5.2 Interventions designed to raise awareness among young people, communities and practitioners
Project Phoenix and the It’s Not OKAY campaign have played an important part in raising awareness of CSE across Greater Manchester. The campaign has developed local information-sharing protocols, education guidance and guidelines around disruption activity. The website includes campaign materials and a range of resources for young people, parents and professionals and can be found at: www.itsnotokay.co.uk
In 2013, the NWG and The Children’s Society launched a national CSE awareness campaign – Say Something If You See Something – targeting businesses (initially hotels) to raise awareness of the signs that CSE activity may be occurring on their premises. It provides risk assessments, posters and training materials to support the safeguarding of young people and children. Training provided to hotel staff in South Yorkshire resulted in a number of incidents being reported to the police and the campaign has now diversified to produce materials for small businesses and taxi drivers among others. More information including links to available resources is available at: www.nwgnetwork.org/say-something-see-something-update
CSE In Plain Sight is a project implemented by Barnardo’s (April 2015 to end of March 2016) and funded by the Department for Education. It focused on raising awareness among those working in the night-time economy (e.g., hotel employees, A&E staff, and security staff) about how to spot the signs of CSE and what to do. The project worked across 12 local authority areas in England, including Manchester, where there was a designated project worker working within Manchester city centre. The project was independently evaluated by the University of Bedfordshire and the final evaluation report was published in 2016 (D’Arcy and Thomas, 2016). It found the project had significantly increased the night-time economy workers’ knowledge about CSE and engagement with safeguarding strategies.
The Pan-London Operating Protocol for CSE (launched by the Metropolitan Police and partners in 2012) brings together a series of procedures on how to tackle CSE for all London Boroughs. It was designed to raise awareness of safeguarding children and young people at risk of CSE and to enable identification of perpetrators and bring them to prosecution. According to a case study review by the Local Government Association (2014: 25-27) the protocol has led to improved awareness of CSE within the community, particularly among hoteliers and local businesses such as taxi firms. The protocol has provided local businesses with training on how to recognise warning signs for CSE and what action to take. Senior engagement across partner agencies has been found to have a significant impact in tackling CSE. A third edition of the protocol (The London Child Sexual Exploitation Operating Protocol) was launched in June 2017 36.
Research on disclosure indicates that increasing the visibility of sexual abuse and exploitation through television story-lines, for example, has helped young people understand that what might be happening to them is not right (Bradley and Wood, 1996). An example is the rise in calls to Childline regarding sexual abuse and exploitation after a 2009 storyline on the soap opera EastEnders that involved a girl being sexually exploited. Similarly, when the Home Office’s This is Abuse campaign (which addressed sexual abuse, violence and rape in adolescent relationships) teamed up with Channel 4’s teen soap Hollyoaks to develop related storylines, this achieved a significant increase in visits to the government’s This is Abuse website (Home Office, 2015).
5.3 Educational resources
CSE is difficult to prevent in the same way that CSA is difficult to prevent: it occurs within perceived friendships or relationships, it occurs with manipulation and coercion, it is not known who the sex offenders are and any child or young person can be targeted. As the field has attempted to prevent CSE, there has been a movement towards education as a preventative method. Education has included formal education within schools and the development of workshops, films, guides, booklets, sessions and activities about CSE, abuse, grooming and relationships.
Whilst it is important that children of all ages (ideally from the earliest age possible) are taught about their bodies and about sex, abuse and relationships, there is in fact very little evidence that education about these issues has an impact on the experiences of abuse or behaviours in relationships or sex (Bovarnick and Scott, 2016), although there is some evidence suggesting it may increase knowledge temporarily. This finding is important because it suggests that education is not a preventative method per se and that increased knowledge does not correlate with reduced victimisation by sex offenders.
Education and participation must be seen as a vital step towards empowering children with information, opinions and attitudes about topics such as sex, porn, abuse, relationships and consent (Pearce, 2009b). However, it is not a solution to CSE and education should not be presented as a tool to prevent children from being ‘at risk’. At best, high-quality education may mean that children disclose experiences of abuse (although more research is needed to support such a supposition).
Relationships and sex education (RSE) provides a crucial platform for education around CSE and should be taking place in both independent and maintained schools (Brook et al, 2014). In their supplementary advice to the government’s guidance on RSE, Brook et al advise that children should be actively taught ‘how to identify behaviour in a relationship which is positive and supportive and that which is exploitative and controlling’ (Brook et al, 2014: 9). Brook provides guidance for teachers and recommends adopting a whole school approach to education around CSE, as well as making sure that a safe learning environment is created. Whilst this is certainly useful, the power dynamics, the process of grooming and the active threats that take place in sexual abuse and exploitation should not be overlooked. Even the most ‘educated’ child can be sexually exploited and abused but still feel, isolated, confused and too scared or too manipulated ever to disclose they are being exploited (Allnock and Miller, 2013). It must not be assumed that increased education is enough to negate the impact and power of a sex offender abusing a child.
Schools are important because, as a universal service, they provide the ideal forum for addressing attitudes and gaps in knowledge. Schools can also be an arena for sexual abuse, exploitation and inappropriate behaviour. In 2016, the Women and Equalities Committee published a parliamentary report entitled ‘Sexual Harassment and Sexual Violence in Schools’, which found that ‘sexual harassment and abuse of girls’ was ‘being accepted as part of daily life’, and that teachers often dismissed sexual harassment as ‘just banter’. It highlighted a YouGov poll 37 from 2010 (conducted for End Violence Against Women), which found that 29 per cent of 16 to 18-year-old girls had experienced unwanted sexual touching at school and 71 per cent heard sexual name calling either daily or a few times a week. The importance of addressing attitudes in the school environment is clear. Schools and communities are where attitudes that condone violence towards girls and women must be challenged, and where healthy, equal and respectful relationships between men and women can be promoted (EVAW, 2011).
As one teacher notes, school offers a chance to make a difference and this brings a moral imperative:
However, there is also research showing significant variation in teachers’ confidence in discussing issues of sexuality in the classroom (Mayock et al, 2007).
Recent reviews of RSE within schools have highlighted the need for more attention to be paid to sexual violence, sexual exploitation and grooming (e.g., Formby et al, 2011; NICE, 2010). Problematically, however, the London Assembly (2015) found that although there was some excellent practice in schools, some schools were not addressing CSE for fear of ‘reputational damage’. So an important message for new service design is the issue of reaching and teaching professionals as well as young people. A project addressing CSE among boys and young men (Yorkshire MESMAC, 2015) found that boys involved in the project wanted more information on grooming and CSE. A small survey of boys from within the cohort involved in the same project indicated a preference for this education to be delivered by trained workers, which could also provide an opportunity to educate teachers.
Although there has been relatively little testing (and even less longitudinal follow-up), educating children about sex and ‘healthy relationships’ through RSE in schools has been highlighted as a crucial preventative factor against CSE (DCSF, 2009; Coffey, 2014; House of Commons Education Committee, 2015). An evaluation of the Sexual Violence Prevention Project from Rape Crisis Scotland (McNeish and Scott, 2015) found that the delivery of workshops to over 8,000 13 to 15-year-olds on issues relating to sexual violence (including consent, the law and use of social media) had an impact on young people’s knowledge. The data suggests workshop sessions were successful in raising awareness of sexual violence, increasing understanding of the importance of equality and consent in healthy relationships and understanding that responsibility for sexual violence lies with perpetrators alone. A third of young people also reported changing their opinions on sexual violence after attending the workshops.
These findings complement those of Bovarnick and Scott (2016) who concluded that these types of session have very little impact on behaviours and actual sexual experiences, but do appear to have some small impacts on knowledge. Because it is so rare to find a programme of education that assesses the retention and application of this knowledge months or years later, evaluative findings – such as the one by McNeish and Scott (2015) – are often based on children being asked to self-report on the day. It is not surprising that after a number of sessions on the topic, most children thought their knowledge had increased. This does not mean the child will retain the information, change any behaviours or not experience abuse or exploitation in the future, however (Bovarnick and Scott, 2016). This is absolutely not to say SRE is not valuable – education may have a number of benefits for individuals, such as giving them the confidence to disclose abuse that has already occurred, or recognising they are harming others with their own behaviours but education around SRE and CSE should not be marketed as reducing risk, reducing CSE or preventing children from being sexually abused. Being clear on the purpose of RSE and wider educative interventions is essential. CSE resources are not themselves preventative – they are educative in nature. They are useful in raising awareness and may support disclosure but cannot prevent an abuser from acting.
The Department of Health and Public Health England (2015) showcase a school nursing case study in which a public health nursing team in Devon identified a number of young people (particularly 13 to 14-year-old boys) who were being sexually exploited for drugs and alcohol. The school nurses had all undertaken a CSE-specific training programme, which helped them identify risks. Young people were discussed at weekly allocation meetings and the school nurses forged links with specialist workers from drug and alcohol services and the missing persons officer at the local child abuse investigation unit, which enabled timely information sharing (as risks could change on a daily basis). They also developed links with schools, offering awareness sessions for staff on CSE indicators and the importance of deploying the MASH enquiry process to raise concerns. School nurses then facilitated joint working between schools and drug and alcohol workers to deliver whole school, targeted and parent information sessions on specific drug misuse (for drugs known to be used in the exploitation ring). The school nurses also gave PSHE lessons to Year 10 and 11 pupils on domestic abuse among young people and CSE (using CEOP evidenced-based resources). Evaluation has demonstrated increased awareness among school staff, parents and carers, and young people. Strategic information sharing procedures have enabled better safety planning for those individuals already being exploited, as well as the early identification of young people at risk of exploitation (DH and Public Health England, 2015: 5). While the result of increased awareness is positive, caution is needed as it is not possible to prove that improved awareness will lead to reduced victimisation of children by sex offenders.
In addition to the importance of being clear on the purpose of RSE, it is also important to be aware of the risks of educative interventions if not delivered carefully. CSE resources – when used with children who have been abused, in particular – can re- traumatise children or induce vicarious trauma. Vicarious trauma can be defined as the feelings of trauma experienced by a third party when witnessing or engaging with the harm or trauma of another. CSE resources now commonly cover the grooming, rape, abuse, physical assault, abduction, drug taking and trafficking of children and are regularly shown to children throughout the UK. Whilst the resources are positioned as educational and designed to increase awareness, there has been no research conducted on whether they cause psychological harm. However, limited research into the impact of children seeing sexually violent content in films and soaps has shown that it can have a variety of effects on children, none of which are positive. Effects include higher levels of aggression, trauma responses and even desensitisation to sexual violence when content is shown to children repeatedly (Villani, 2003). Much more research is required in order to understand the psychological impact of showing videos of sexual abuse and sexual violence to children as an educative response. It is important to reflect critically on the content being shared with children and young people, and ask whether the proposed benefits of sharing disturbing materials have any evidence of positive impact.
A further point about the use of CSE resources in universal education and in one-to-one support was highlighted initially by the report from the Women and Equalities Committee (2016). It raised concerns that resources related to sexting in particular are being used with children and young people, asking children to consider what the victim could have done differently, who they should have told and what they should have done to protect themselves. This is problematic, as it reinforces victim-blaming narratives and there is a concern that children are being taught that responsibility for harm lies with the victim. Relating this to practice in CSE, it is vital that any conversations or exercises about children being sexually abused focus on the actions, motivations, methods and decisions of the sex offender and the impact on the victim – rather than the actions, motivations and decisions of the victim. Skilled professionals, with a robust content quality assurance process, and the space to critically reflect on how educational resources can be used ethically are three essential considerations for any local area planning to implement educational interventions.
Reflection pointers
- What are specialist services doing locally to support schools to build their knowledge, skills and confidence in relation to RSE, so that they play the most effective role possible?
- How can we ensure that the expertise and accessibility of school nurses is being used to good effect?
- What role might local strategic safeguarding arrangements have in encouraging schools and other universal services to engage with CSE prevention?
- How can we assure ourselves that educational resources and interventions focus on the actions, motivations, methods and decisions of the sex offender and the impact on the victim – rather than the actions, motivations and decisions of the victim?
- Are we clear, in our strategy and in our communication, that education is valuable in a number of ways but that it cannot stop abuse and exploitation?
- How do we ensure we are capturing the impact of educational activity (included unintended negative consequences?
- What are we doing to ensure those delivering educational interventions are appropriately skilled, supervised, able to reflect critically and attuned to the potential risks?
Using educational resources appropriately
Before using an educational resource regarding CSE, it is important to reflect on a number of issues:
- Many CSE resources depict rape, abuse, harm and distress. It is vital that great care is taken when using these resources with any child or group of children. These resources are not suitable for children with histories of trauma and abuse or children who are being exploited or abused currently, as they may re-traumatise a child.
- Many CSE resources are not suitable for children with learning disabilities and they cannot be simply ‘adapted’; however there is a wide range of CSE and PSHE resources for children with learning disabilities produced by organisations such as BILD.38 There is also guidance on how to work with disabled children around CSE and RSE in Barnardo’s practice guide for professionals (Smeaton et al, 2015).
- Children should not be repeatedly exposed to CSE resources depicting child abuse as this may cause vicarious trauma.
- When resources are used in schools, there must be ample and ongoing wraparound support for the children during and after the resource is used.
- Resources should be used with care to ensure that children are not taught that responsibility lies with the victim
- Those delivering educational activity must be well-trained, highly-skilled and able to reflect critically on the messages being delivered and the potential impacts of educational resources.
5.4 Building resilience, building relationships and early help
Discussing relationships and resilience in the context of early help is not intended to imply that relationship building and a focus on resilience are not important aspects of other more specialist forms of intervention. Relationship building is, of course, essential across the range of interventions offered to young people.
Resilience
However, a key factor in the early intervention and management of young people at risk of or experiencing CSE is the assessment and development of resilience (DCSF, 2007). Essential enablers of resilience include self-esteem, self-efficacy, positive attachments and support networks (including family, institutional and community based) (Glover, 2009; Newman, 2004). Resilience can also be built through cognitive training and curriculum-based models such as the Penn Resiliency Program (Gillham et al, 2007), which have reportedly been applied to treat depressive symptoms in school children in the USA and more recently in the UK (Department for Education, 2011).
A young person’s resilience to sexual exploitation may manifest itself through coping strategies that may not be positive in terms of outcomes. As Dodsworth (2014) points out, behaviours may be both adaptive (such as reflection, seeking support or disclosure) and maladaptive (for example, substance misuse, running away, resistance to help from professionals, self-imposed isolation or staying in contact with an exploiter who may provide consistent resources and affection and a ‘least worst option’ for meeting needs) (Hallett, 2015). And as we saw previously, practitioners may risk misinterpreting coercion as ‘choice’ (Lebloch and King, 2006); maladaptive coping strategies may give the appearance of assertive ‘choice’ when in fact they indicate a child’s highly constrained life experience or a maladaptation to previous harm or adversity.
The challenge of working with young people who are resistant to, or suspicious of, adult intervention may be reflected in their treatment at the hands of professionals. Griffiths (2013) points out, in the serious case review (SCR) of several young girls subjected to sexual exploitation (similar messages are found in other SCRs), that there is a tendency for agencies to frame these young people as problematic and a well-intentioned focus on changing their behaviour (or adopting didactic approaches such as explaining risk and threats) served to make them feel disempowered and push them away from seeking help. Viewed through the lens of building resilience, such an approach provides neither self-esteem nor self-efficacy, nor a secure network. Those elements are dependent on building a meaningful relationship with the young person, which service responses can sometimes undermine through short-term casework, structural boundaries and the application of thresholds, etc. Similarly, the Coffey Report (2014) highlighted the frustration of young people in care who tended to view social workers as a transient presence who could be judgmental; this adds further emphasis to the importance of relationship-based practice.
‘Being there’ for young people and building a relationship is the most effective professional approach for building resilience (Coleman and Hagell, 2007). Newman (Research in Practice, 2014b) also suggests that a family-centred approach that addresses the most proximal relationships (the relationship between parent/carer and child, for example), focuses on building strengths rather than identifying weaknesses and harm, and includes the views of young people when considering interventions, is key. Newman also points out that professionals have a tendency to focus on the most acute stressors in a young person’s life rather than the chronic ones (such as peer pressure), which may be a significant source of stress for the child. Considering the everyday pressures faced by young people alongside more major issues may be useful in both establishing resilience and reducing risk.
For children and young people in care, staff attitudes are a critical factor in building resilience, wellbeing and managing risk (The Care Inquiry, 2013). According to Berridge et al (2012) children and young people living in residential homes value:
- Consistent attitudes and responses to any antisocial behaviour and incidences of going missing
- Having someone to talk to
- Recurrent activities that involve both staff and other resident young people.
It is also worth noting that the Chief Medical Officer’s Report (2013) emphasises the need for schools to play a key role in developing resilience and wellbeing and clearly states the case for high-quality PHSE and SRE education as a means of doing so.
There are challenges in relation to engaging these children and young people and therefore in building a successful relationship. Some may have underlying attachment difficulties in relation to their families. (However, caution must be applied here; Shemmings and others highlight that language matters – ‘attachment’ implies a condition or problem, whereas ‘relationships’ affect us all. See Research in Practice, 2016b.) And as highlighted previously, young people affected may not recognise themselves as ‘victims’ and may resist being ‘rescued’. Young people often return to those who are abusing them. It is important, then, to contextualise the issue of CSE in terms of the young person’s experience of the difference in ‘relative power’ between a well-intentioned professional and a person seeking to exploit them. The latter may have ‘street status’ and is likely to be able to offer money, gifts and 24-hour availability and may resort to violence; the practitioner is less compelling in comparison. A bullied child who is hungry and afraid may get food or money from their exploiter who may be perceived as providing safety; in contrast ‘all they get’ from their therapist/worker may be a session, which is of less instant use (Royal College of Psychiatrists, 2012). The RCP (2012) argue, therefore, that what is required are outreach interventions, interventions that are relevant to young people, and treatments that involve and integrate different approaches (including mental health services, parenting, education, physical health and peer-group relationships).
Closely connected to promoting a child or young person’s resilience is the notion of self-efficacy. Practice must be participative and tenacious in its efforts to re-establish a sense of control (Warrington, 2016; Research in Practice, 2017) if experiences of exploitation are to be addressed healthily. See Section 7 for more discussion on participation.
Establishing and sustaining relationships with young people also has implications for staff retention and structures, as well as for staff emotional wellbeing (see Section 8 on workforce considerations).
Reflection pointers
- What are we doing to promote resilience in young people at risk of CSE? How is participatory practice enabled in our local services?
- How do we ensure that our service structure and systems enable practitioners to develop and sustain positive and trusting relationships that can build resilience?
- Might we be inadvertently undermining resilience through any (well-intentioned) practices?
- What are we doing to ensure that practitioners themselves have the support they need to help them cope with emotionally difficult situations?
- How do we attract and recruit practitioners who are resilient and can work effectively within complex situations and relationships?
- And how do we, as an organisation, promote and maintain practitioners’ resilience?
Key messages
- The transformative power of positive relationships is crucial when working with young people who have been harmed.
Building a strong, respectful and supportive relationship is integral to effective intervention. - Professionals do need to exercise caution when using the notion of resilience. Some behaviours might be mistaken for signs of resilience when in fact that young person is asking for help; equally, some behaviours may be viewed as ‘bad’ when in fact the young person is demonstrating a form of resilience to the trauma they are experiencing.
- Practice that is participatory can promote self-efficacy and therefore resilience.
Early help
The evidence for preventative interventions and the value of educational resources was considered earlier. Providing help at an early stage can reduce the risk of harm, and some examples are offered below. In many ways, the demarcation between early help and support for medium-risk young people is blurred – and as with early help more generally, there are not precise boundaries in relation to early help and CSE. To that end, this short section on early help should be read in conjunction with the earlier section on preventative approaches (see Section 5.3) and later section on supporting young people at high and medium risk (see Section 5.5).
Barnardo’s evaluation of its services for young people vulnerable to and experiencing sexual exploitation has found that their interventions are effective in reducing the risk of CSE and connected risk behaviours (Barnardo’s, 2011b; Scott and Skidmore, 2006); further – independent – research is needed to corroborate these findings, however.
At the point of publication, each of Barnardo's specialist CSE services operates its ‘Four A’s’ approach, which provides a potential template for engagement and the provision of early help:
- Access: Providing easy access to services, with referrals accepted from a range of agencies and young people often having the option to self-refer.
- Attention: A dedicated key worker remains with the young person throughout their involvement with the service, offering a consistent relationship and support.
- Assertive outreach: Staff use a range of techniques to engage young people and to help them access support; with young people who show little interest, the support worker’s persistence helps to demonstrate genuine concern for the young person’s wellbeing.
- Advocacy: Supporting young people to gain access to other key services and to stay engaged with them, including providing help to keep appointments. The support worker will also act as an advocate if the young person’s relationship with a service breaks down. (Barnardo’s, 2011b: 7)
5.5 Working with children at risk of, and those experiencing, CSE
With this category, there may be an immediate risk or actual incidences of involvement in CSE. It is common across the UK to categorise these children as ‘medium-high risk’ rather than victims. For clarity, this review only uses the language ‘at risk’ to mean children who are at risk of being sexually exploited and uses ‘victim’ where there are actual incidences of grooming or exploitation of the child.
Children who are victims of, or at risk from, CSE can also be ‘harder to reach’ (or, rather, may find professional support harder to access) – for example, young people without secure home lives, supportive adult relationships or consistent supervision. From a strengths and needs perspective, it is important to consider carefully the resources and strengths available to young people to help them move away from high-risk situations before considering therapeutic or educational interventions. For example, Smeaton (2013b) points out that when working with young people who experience both running away and CSE it is crucial to ensure they have their most basic needs net. This might include providing facilities to wash and eat and ensuring that the young person has a safe long-term place to stay to help prevent them returning to an exploitative situation to meet those needs (such as being given somewhere to stay in return for sexual exploitation). Smeaton (2013b) also stresses the importance of building trust and providing consistent caseworker contacts and lengthier interventions to address the long-term impacts of CSE.
This view supports research by Railway Children (Thompson, 2014), which identified two very distinct trajectories for children who run away from home or are made homeless. Young people who make a circular journey (i.e., from leaving to returning home) may benefit most from support that improves safety and relationships within the home. Young people on linear journeys may not return home (or may not have the possibility of returning home) and so need more support to live independently. Thus there may need to be more focus on ‘non-procedural’ elements of identifying CSE, such as multi-agency working and working with children and families post disclosure.
Where young people who are victims of, or at risk of, CSE are placed away from home, it is necessary to ensure their carers have appropriate skills and support. An example of this is the Barnardo’s model of specialist foster care placements for those young people who had been victims of sexual exploitation or trafficking (Shuker, 2013b). This small-scale study showed that foster carers were trained to have a basic knowledge and understanding about child exploitation and child trafficking as child protection issues; this covered the impact of exploitation and trafficking on the young person, resulting behaviours and vulnerabilities, and an understanding of the need for multi-agency working. Placement outcomes included foster carers employing a range of safety strategies as a result of their training. In 9 of the 12 placements tracked, foster carers successfully kept children safe from exploitation. The young people reported feeling safe and warm and trusting relationships developed between them and their foster carers. Improved physical and psychological wellbeing was observed in those young people in medium to long-term placements. It must be noted, however, that this study did not track the progress of children in regular foster placements as a control group in order to look at whether the improved wellbeing was related to the specialist foster carers.
In addition to specialist support for the CSE itself, ‘high-risk’ young people may also need a range of specialist support to address the impact of CSE. As described by Williams and Watson (2016), depression, dissociation, self-harm, eating disorders and the misuse of drugs and alcohol are all common ways in which people may ‘manage unbearable feelings of terror, anger, fear, profound sadness, shame and loss when they have limited control and when they do not feel entitled to speak, or safe enough to do so’ (Williams and Watson, 2016:6). Recognising these symptoms as a response to trauma, and ensuring that the experience of CSE is not obscured by the resultant symptoms, is important.
As services become more specialist, particularly where these services attempt to deal with highly problematic behaviour, there is a need to consider whether services remain appropriate for children and young people across their life course. Thornberry et al (2010) suggest that many interventions for adolescents are either ‘downward extensions’ of adult programmes or ‘upward extensions’ of programmes designed for children, while young women are frequently thrust into equally inappropriate services geared to adults (Burman and Batchelor, 2009). To this end, those responsible for commissioning and delivering specialist interventions must ensure that the programme or service is appropriate for young people and is designed in a way that responds to the specific needs of this age group.
Of critical importance is the need to ensure services and support are tailored to the needs of children. This includes making sure services are designed for adolescents and their growing sense of autonomy, whilst maintaining a clear message that young people are not responsible for the harm they experience. This last point has particular implications for those working within the justice system. Age-appropriate practice and processes, which honour a victim’s self-determination and provide opportunities to exercise autonomy are called for in a recent report by Barnardo’s ‘Journey to Justice’ (Marsden, 2017).
Warrington’s work (Research in Practice, 2017) highlights the importance of participatory practice within CSE, explaining that many young people using CSE services or engaged in related criminal justice processes report experiencing a loss of control and increased stigma, often linked to poor communication and exclusion from decision making. Services involved in supporting young people affected by CSE therefore need to consider carefully how to avoid replicating the disempowerment that characterises exploitative relationships. Professionals responding to CSE from all agencies must be committed to listening to young people and engaging them in decision-making processes, as recommended in national guidance (Beckett et al, 2017).
Warrington notes that:
Participation is described by Warrington and others as a key facet of an effective protective response. There is emerging evidence that participatory approaches support young people’s long-term recovery from the impacts of abuse, acting as ‘part of a process of recovering their sense of self, and sense of agency’ (Brodie et al, 2016).
For a more detailed discussion on participatory practice with children and young people affected by CSE, see Warrington’s Frontline Briefing for Research in Practice (2017): ‘Young person-centred approaches in CSE - promoting participation and building self-efficacy’. (Participatory practice is also explored in Section 7 of this scope.)
Reflection pointers
- Do we have a clear vision of what a needs-focused and user-led service would look like?
- Do practitioners recognise the basic needs of high-risk young people (e.g., young people who run away) or are plans drawn up too hastily before a young person has been stabilised?
- Are we confident that specialist services, particularly mental health services, ‘see’ the whole young person and their experiences – or do the symptoms of distress inadvertently obscure this?
- How do we ensure that CSE services and practice are tailored to the individual needs of children and young people? To what extent is our practice and service delivery truly participative?
- What support do practitioners need to enable them to work alongside children in a way that is meaningfully participative?
5.6 Therapeutic and trauma-informed interventions
The connections between sexual abuse and other forms of trauma are complex and widely documented. Whilst not all CSE victims will have experienced earlier trauma, previous forms of trauma have been linked to increased risk of CSE (Kaestle, 2012; Reid, 2011); childhood sexual abuse in turn is linked with a wide range of common mental disorders, including depression, anxiety disorder, phobias, alcohol and drug misuse, post-traumatic stress disorder and eating disorders (Jonas et al, 2011).
While being clear that not all CSE victims (nor perpetrators) will have experienced CSA, it is important to look at the connections: young women who have been sexually abused have been reported to be at increased risk of engaging in high-risk sexual behaviour (Farmer and Pollock, 1998) and experience higher rates of sexual re-victimisation (Nelson et al, 2002). Some studies suggest that growing up experiencing family violence combined with experiencing sexual abuse may increase the risk for some young men of subsequently abusing others (Skuse et al, 1998). Longer-term prospective studies are needed here, however, and the assumption that young people perpetrating abuse have themselves suffered sexual abuse is widely contested (Hackett, 2016). The relationship between CSA, later sexual exploitation and (for women in particular) sexual abuse into adulthood has been explored by a number of researchers; see Lalor and McElvaney (2010) for a useful discussion on how these experiences may be linked in a person’s life. Violent and abusive experiences are a predictor of subsequent psychological and emotional difficulties and contact with mental health services (Abel et al, 2012, cited in Williams and Watson, 2016). Trask et al (2010) consider the wealth of research studying the effects of CSA, highlighting post-traumatic stress disorder (PTSD), anxiety, aggression, suicidality, depression and behaviour difficulties in particular.
When humans experience extreme stress, it makes sense that their responses may be seen as extreme. When humans experience repeated interpersonal traumas and serious crime, they are likely to be distressed, which may manifest in diverse ways for each person (Giller, 1999). The importance, then, of trauma-informed interventions is clear. They can be understood as therapies designed for survivors of abuse (particularly sexual abuse) in which trauma-related symptoms are seen as legitimate and rational reactions to abusive situations. Unfortunately the evidence for effectiveness of such interventions for CSE is scarce; however, useful messages can be drawn from related literature, including that covering CSA and mental health. One recent report from Australia (Quadara and Hunter, 2016) provides a comprehensive exploratory study into the way trauma-informed approaches can be used to support children who have been sexually abused. It listed the key principles for any organisation wishing to be trauma-informed in their approach.
These are listed below along with principles based on other sources:
- Having a sound understanding of trauma arising from interpersonal violence and abuse and the impact on the life of the child and the family surrounding them
- A system-wide understanding of abuse, violence and victimisation in the lives of people with mental health issues and using that understanding to design the service
- Ensuring that the procedural, organisational, operational and direct service provision promotes psychological and physical safety rather than undermines it
- Ensuring strengths-based approaches are emphasised, encouraging autonomy and collaboration
- Being responsive to the lived experiences of the children, including their context, their sex, their ethnicity and culture
- Ensuring professionals (and those close to the victim, where appropriate) understand trauma responses during and after a sexual offence (this will include countering some of the assumptions as to what constitutes the ‘right response’ to rape and sexual assault)
- Recognising the reasons and processes underpinning the trauma responses to sexual victimisation
- Ensuring trauma behaviours are understood in context and not interpreted as unrelated mental health or behavioural issues, or ‘disorders’.
(Quadara and Hunter, 2016; Payne et al, 1999; Lodrick, 2007; Möller et al, 2017)
Cognitive Behavioural Therapy (CBT) and Dialectical Behaviour Therapy (DBT) and its use with CSE
In the context of ‘treating’ children who have experienced CSA, cognitive-behavioural approaches:
In addition, work is undertaken to address learning and behaviour such as aggression or ‘acting out’, anxiety, self-blame or sexualised behaviour. CSA-focused CBT usually takes the form of short-term highly structured intervention sessions, often alongside techniques to ‘practise’ in between contact time with the CBT practitioner.
It has been reported that CBT may be effective in reducing psychological harm in children exposed to trauma (Wethington et al, 2008), including PTSD, anxiety and depression. This finding was supported by Trask et al’s (2010) meta-analysis of the treatment effects for CSA. They found that cognitive-behavioral interventions were more beneficial than treatments based on ‘other’ theoretical models. Individual and group treatments were found to be equally effective, while studies seemed to show greater effectiveness with older children and with males. That older children may benefit more from treatment makes sense given that many existing interventions require the child to understand ‘cognitive components’ (e.g., the cognitive triad, cognitive distortions). This suggestion would tally with evidence that cognitive therapy techniques may need to be adapted for younger children (Doherr et al, 2005). Ethnicity was not a factor in treatment effectiveness.
In their systematic review of CBT to address the impact of CSA, Macdonald et al (2012) agree that cognitive-behavioural approaches warrant ‘consideration as a treatment of choice for sexually abused children who are experiencing adverse consequences of that abuse’. However, they warn that whilst there is relatively consistent evidence that cognitive-behavioural approaches may lead to reductions in depressive, anxiety and post-traumatic stress symptoms in children, this evidence is weaker than most studies have suggested. Similarly, Allnock and Hynes (2012) highlight the limited number of evaluative studies conducted, the varied methodological quality of those that do exist and the existence of unanswered questions around the optimum timings for interventions and reliability of outcomes for ‘patients’.
There is emerging research to suggest that Dialectical Behaviour Therapy (DBT) may be useful in the treatment of adolescents who have suffered abuse. DBT is a specific form of psychosocial-oriented CBT that is:
- Support oriented and focused on helping a person identify and build their strengths
- Built around regular collaborative therapy sessions, which pay attention to working through problems in relationships, role- playing interactions and developing communication strategies and skills for managing emotions.
DBT was developed by Linehan (1993) to be used in the treatment of ‘borderline personality disorders’ 39 and is also applied in complex trauma-related issues. The therapy builds on the notion that conflicting emotions can exist in a person at the same time. It has been increasingly used with adolescents, in particular those experiencing mood lability, impulsivity and engaging in ‘high-risk behaviours’, or who are prone to self-injury (Rizvi et al, 2013).
Oxfordshire and Buckinghamshire Mental Health Partnership NHS Trust (Alfoadari and Anderson, undated) provide a DBT service to looked after children, including those exposed to domestic violence, sexual abuse or exploitation. Case studies of patients who used the service revealed reductions in self-harm and improved stability of mood and engagement in education.
An evaluation of DBT for looked after adolescents with repeated serious self-harm (James et al, 2011) also found that DBT was successful in reducing elements of depression, hopelessness and self-harm in around three-quarters of patients. However, 35 per cent of ‘patients’ did not engage, suggesting that the treatment cannot be assumed to be effective in all cases and highlighting the importance of taking an individual approach to the assessment and treatment of young people that recognises the diversity of their needs and strengths.
In terms of service development, barriers to the provision of therapeutic services must also be considered, such as the need for specialist assessments, referral time and added costs (including establishing which agency will be responsible for those costs), and the engagement of young people who may be resistant or who find it hard to engage with professional support. Professionals may also face resistance from caregivers. For looked after children, uncertainty around the length of a particular placement may also be a barrier to longer-term service referrals.
The issues that young people can face as a direct result of being abused and exploited can re-emerge later in life and local areas are encouraged to ensure post-abuse support services are available (LGA, 2014). Interventions should not be offered on a short-term basis but for the requisite period of time that the young person needs; this may be costly, but re-referrals and cyclical crises are arguably more so. Ofsted (2014) found that referral pathways to therapeutic support were not always well developed and that cases involving work with CSE victims are closed too soon. There should be joint commissioning arrangements for health, social care and education and common thresholds for interventions across agencies with clear referral pathways and, where possible, pooling of budgets, to enable smoother and more fluid access to support.
Reflection pointers
- Do we interrogate the theoretical basis for the therapeutic interventions we commission?
- How are practitioners supported to develop their skills and knowledge to provide trauma-focused interventions?
- How do our commissioning arrangements enable, or impede, therapeutic support being offered to all those who need it?
5.7 Interventions with families
Parents, families and the wider community can play a crucial role in safeguarding and in the identification of CSE (Scott and McNeish, 2017). In a recent Children’s Society poll (Pona et al, 2015) half of 16 to 17-year-olds said that support from families was a key factor in helping them to resist pressures to ‘take part in risky activities’. However, a third did not feel supported by their families ‘in most things they did’.
In practical terms, parents may not always have the knowledge or support to safeguard their children in every situation. For example, an evaluation of The Children’s Society’s Self project in Torbay (Smeaton, 2014) revealed that, in the case of children who run away from home and are vulnerable to CSE, some parents did not know how to report their child to the police as missing and some got a negative response from the police when they did.
A Barnardo’s pilot project (Families and Communities Against Sexual Exploitation – FCASE) aimed to address how professionals working within and with the voluntary sector can best work to raise awareness of CSE among families and young people at risk of CSE. An evaluation by D’Arcy et al (2015) identified key mechanisms for change through which outcomes from direct work were achieved; these included:
- Having practitioners who were experienced in working with CSE, but also skilled in mediation (due to the high level of family conflicts experienced) and were adaptable to the family’s needs.
- Practitioners worked with parents, responded to their concerns and allowed them to reflect on their experiences. They did not simply dispense information.
- Service users found the less formal approach of the voluntary sector workers put them at ease. This flexibility of the voluntary sector to ‘reach out’ to families and engage in a holistic family-based approach demonstrates the benefits of multi-agency practices. (D’Arcy et al, 2015)
Qualitative evaluation of the project found that families and young people both felt more able to identify CSE and associated risks as well as to discuss experiences and concerns together. In some cases this also improved relationships between parents and young people.
The Children’s Society’s Safeguarding Children at Risk – Prevention and Action (SCARPA) Programme supports young people who go missing from home in the Newcastle area. Between 2009 and 2011, the project deployed a family worker to provide tailored and flexible support to families of young people involved with the programme, offering a listening service, guidance and family mediation. A qualitative analysis involving parents (Medforth, 2011) found that some parents felt increased confidence in their parenting skills and communication within the family, and reported improved relationships with children as well as increased family stability. Crucially, some parents also reported having to overcome fears or negative past experiences to engage fully with the programme. Professionals highlighted that building trust with parents as well as children was crucial to the success of the intervention.
In their relational safeguarding model, PACE (2014) advises taking a partnership approach with parents towards safeguarding children against CSE. PACE also stresses that the exploitation and abuse suffered by a young person may distort the perception they have of their parent(s) and create tensions, including between parents or carers; this needs to be addressed to safeguard the child successfully. In some local areas PACE provides a full-time parent support worker to assist the local multi-agency CSE team, working exclusively with the parents of the child. This can act also as a form of mediation between parent and child if tensions exist.
These messages are echoed in a recent evidence review produced by the Centre of Expertise on Child Sexual Abuse. The authors explain that parents want respectful, honest relationships with professionals, and to develop their ability to safeguard their child, rather than to be blamed or stigmatised (Scott and McNeish, 2017). The go on to set out the four key areas within which parents are likely to need support:
- Their relationship with their child, and particularly understanding teenage development, what makes their child vulnerable, how perpetrators groom and control, their role as parents, and how parenting can help.
- Their own emotional needs, including dealing with the trauma of CSE, the impact of their own past experiences, and parents’ relationships with each other.
- Dealing with systems, including understanding how police, legal and child protection systems work, and having someone who can advocate for parents.
- Building their resilience, including identifying sources of support in the wider family and community, and accessing the professional and peer support they require.
(Scott and McNeish, 2017:5)
Reflection pointers
- How well are we working with parents and families? Are we providing a systemic and strengths-based approach wherever possible?
- How empowered do parents and carers feel by our support? Are we inadvertently blaming or stigmatising parents and carers? Under what circumstances are family-based interventions proving most useful for young people? How do we capture this?
Key messages
- Providing help at an early stage can reduce the risk of harm.
- It is important to consider carefully the resources and strengths available to a young person when planning support and services.
- Young people may need to be stabilised before therapeutic interventions can be offered – for example, they may need help to move away from a high-risk situation, such as being homeless, before considering therapeutic or educational interventions.
- Building trust and ensuring consistency of caseworker contact are necessary to sustained interventions to address the long-term impact of CSE.
- Therapeutic trauma-informed interventions are an essential part of overall service provision for young people who have experienced CSE. They can be understood as therapies designed for survivors of abuse in which trauma-related symptoms are seen as legitimate reactions to abusive situations.
- For older children who have experienced abuse, there is some evidence for the benefits of Cognitive Behavioural Therapy (CBT) (both individual and group) and Dialectical Behaviour Therapy (DBT). However, the evidence base for DBT is not yet robust, and the evidence base for CBT may not be as robust as has been widely assumed.
- Treatment cannot be assumed to be effective in all cases. This highlights the importance of taking an individual approach to assessment and treatment, one that recognises the diversity of each young person’s needs and strengths.
- The issues that young people can face as a direct result of being exploited can re-emerge later in life. Interventions should not be offered on a short-term basis but for the requisite period of time the young person needs; this may be costly, but re-referrals and cyclical crises are more costly.
- Practice with children and young people affected by CSE must be as participatory as possible, providing opportunities to regain a sense of agency, autonomy and self-efficacy.
- Having practitioners who are experienced in working with CSE but also skilled in mediation will help engage families in a holistic family-based approach.
- Parents value having practitioners who respond to their concerns, allow them to reflect on their experiences and do not simply dispense information.
- Parents can experience professional intervention as blaming or stigmatising.
6. Multi-agency working and information sharing
Although the principle articulated by Beckett above is increasingly accepted, it is not always applied in practice. In her review of the work of Local Safeguarding Children Boards to protect children from sexual exploitation, Pearce (2014) found that some youth and health services were not recording or sharing information with child protection services because of concerns over confidentiality, while some police forces were recording data only in certain circumstances, for example, as part of a targeted operation. The mix of roles, responsibilities and recording practices meant that, when surveyed, data on CSE was at best disparate – and therefore not helpful in identifying risk and facilitating preventative responses.
Smeaton (2013b: 62-65) outlines a number of factors that professionals have identified as supporting effective multi-agency work in addressing CSE, including effective links between the police, social workers, schools, healthcare professionals and the voluntary sector. However, effective links are dependent on communication and formal opportunities for information sharing. Moran et al (2007) discuss this in relation to early intervention support teams. Regular inter-agency meetings were seen as significant in facilitating communication and understanding of what each team was doing and to address practical issues, such as referrals and case-recording procedures. In other contexts, the co-location of multi-agency teams, healthcare professionals and sexual health clinic staff based within specialist projects has also proved useful, and co-located Multi-Agency Safeguarding Hubs (MASHs) are now common within local authorities (Brooks and Brocklehurst, 2014).
As mentioned earlier in this scope, Project Phoenix (2014) is a collaboration of public and third sector partners who have come together across Greater Manchester to tackle CSE and offer a possible model for other areas to follow. There are specialist teams in each of the ten districts of Greater Manchester offering a joined-up multi-agency and integrated response to dealing with CSE, and all key stakeholders work to a standard set of guidelines and operating procedures. The establishment of Project Phoenix followed extensive scoping with relevant stakeholders by the Greater Manchester Safeguarding Partnership (GMSP) in 2012. GMSP published a broad overview of the current response to CSE in Greater Manchester, including an analysis of the key risks and opportunities faced by all parts of the system. Partners to GMSP formally committed to developing a response strategically, tactically and operationally. Senior members of partner agencies (including Directors of Children’s Services, the police, the Crown Prosecution Service, St Mary’s Sexual Assault and Referral Centre, and the Association of Greater Manchester Authorities) met and agreed a common priority to tackle CSE together, from prevention to long-term therapeutic support, including disruption and effective prosecution where appropriate 40. Similar ‘joined-up’ examples to that pioneered by Project Phoenix in Greater Manchester are now being seen elsewhere.
In order to achieve consistent inter-professional responses to the identification and management of CSE and to establish preventative interventions, close consultation is required between agencies. The unique contribution of each agency should be recognised and enabled. Schools are a crucial arena for the establishment of preventative education and for the early identification of risk. Health has an equally vital role to play – whether it is frontline A&E staff identifying at-risk young people or mental health practitioners supporting recovery, the key is to view the child as an individual and not ascribe a medical model to their needs. Voluntary sector organisations are often uniquely placed to employ creative methods and to provide sustained support over time.
Problem profiling
Interventions must focus on creating a step change in response. At a strategic level, it is important to assess and identify local patterns of CSE (problem profiling) and amend interventions to reflect the local picture. There is limited evidence nationally as to what constitutes a good problem profile but local guidance tends to suggest it should:
- Bring together all the known intelligence and relevant data held across different agencies to inform strategic decision making and local practice development
- Have clear terms of reference and a clear plan for data collection formulated for each agency detailing what is required from them
- Include third sector and voluntary sector organisations as well as statutory and non-statutory public sector organisations
- Identify intelligence gaps
- Help to identify the known extent of the problem and identify where resources should be targeted.
The problem profile will require collective ownership across all partners to support its development and a committed and effective analyst to review key findings and identify intelligence gaps (OCC, 2013a; LGA, 2014). In Rochdale the problem profile has been used successfully to target interventions and the analyst received a national and international award 41.
There are potential limitations to local area ‘problem profiling’, however. It can present CSE as a geographical issue and so is mapped on to areas as ‘hotspots’. This fuels potentially unhelpful assumptions: that CSE is geographically situated in some areas and not others, that CSE is unlikely to span many areas at once (exploitation on the internet and in wider trafficking cases is not limited by local boundaries, for example) and that CSE is qualitatively different from CSA, which is perceived as happening everywhere at all times.
There has been a call to ‘always assume that CSE is occurring in every area’ (Coy et al, 2017; Beckett, 2013) so it is right to be cautious of identifying ‘hotspots’ and ‘problem areas’ within local authorities, as this can lead to the significant increase of resourcing in some areas and not others. An unintended consequence of oversimplified ‘hotspot’ and problem profile mapping would be an area that identifies a certain place in which CSE is occurring and restructures its resources and teams around that area, leading to an increase in referrals and disclosures for that area and a decrease for those areas from which resources have been diverted. This results in circular thinking and reinforces the myth that CSE occurs in certain areas and not others, with local statistics seemingly confirming the ‘hotspot’.
Reflection pointers
- Are we making best use of the specific skills of each agency across our area?
- Are we allowing professional hierarchies to dominate, rather than working to our strengths?
- Have we undertaken effective problem profiling? Or do we need to exercise more caution in relation to what we find? Are all partners locally committed to taking collective action on its findings?
- Are we alert to the potential limitations of problem profiling? Do we have the right checks and balances in place to avoid oversimplified understanding?
7. Young person-centred practice and participatory approaches
The UK now has an established discourse of participation in public service development and delivery, albeit that these words are not always matched by action. Efforts to involve young people in both decision making about their own lives and in the creation of new services are to be welcomed. This section is concerned with the evidence supporting user-centred practice and the development of services with young people as participants in the developmental process. The evidence shows that high-quality participation which enables young people to contribute effectively to their personal progress or to the development of services that meet their needs, results in higher levels of personal resilience and confidence. For young people who have experienced sexual exploitation, this is critical to their formation of a sense of self that is apart from their feelings of victimhood. This premise was central to the Wigan and Rochdale Child Sexual Exploitation Innovation Project, resulting in the creation of ACT 42.
In terms of service design, there has been a trend in professional responses to CSE towards service models that are both needs- focused and user-developed – in other words, towards children being directly involved in service design and response (HM Government, 2015b). Ofsted has showcased Street Safe Lancashire (Ofsted, 2013a) as a good practice example of involving children and young people in the design and development of CSE services. The Lancashire Safeguarding Children Board (LSCB) brought young people together who had accessed CSE services to produce a guide Standing Tall After Feeling Small (Children’s Society, 2013), which set out their needs, concerns and experiences in their own words. The guide instructed practitioners on ‘how not to work with young people’. It led to a review of LSCB training for professionals on CSE, operating procedures and action planning.
The legislative background to young people’s participation
It is now commonplace for children and young people’s services to involve users in service development and delivery. And it is well understood that any child or young person in receipt of any kind of care that involves any form of decision making about their welfare, should be involved in the decision-making process to a degree that matches their capacity (Fleming, 2013). This support for children and young people’s participation in decision making and service design is the result of three decades of policy-making and practice development in the public and voluntary sectors. Legislation enacted in the UK over the last 25 years has created a common assumption that the participation of children and young people is both beneficial and essential (Tisdall, 2008).
The Children Act 1989 is one of many key pieces of government legislation and regulation that establishes the right of children and young people to have their ‘wishes and feelings’ taken into account in decision making about their future. This principle is carried forward throughout the Act’s implementation guidance, ensuring that mechanisms are in place to enable children and young people to have some input into decisions being made on their behalf.
Section 3(5) of the Childcare Act 2006 states that, in relation to early childhood services:
A significant instrument underpinning children and young people’s participation in the public sphere is the UN Convention on the Rights of the Child (UNCRC). Agreed in 1989 and ratified by the UK government in 1991, the UNCRC requires the government to account for its progress against 54 articles set down within it and ‘have regard’ for the Convention when developing policy affecting children and young people (see Council of Europe, 2012). Article 12 of the UNCRC is concerned with the right of children to participate in decisions that affect them. It states:
This article underpins much of the theory and practice of ‘participation’ that has been established since the UK government ratified the Convention.
Models of participation
Youth work practice has been particularly influential in the development of participatory approaches, based as it is on principles of voluntary participation, relationship and association (Smith, 2002). In its document Ethical Conduct in Youth Work, the National Youth Agency defines the nature and purpose of youth work:
The purpose of youth work is to facilitate and support young people’s growth through dependence to interdependence, by encouraging their personal and social development and enabling them to have a voice, influence and place in their communities and society.
Youth work is informed by a set of beliefs which include a commitment to equal opportunity, to young people as partners in learning and decision-making and to helping young people to develop their own sets of values. We recognise youth work by these qualities (based on Davies, 1996):
- it offers its services in places where young people can choose to participate
- it encourages young people to be critical in their responses to their own experience and to the world around them
- it works with young people to help them make informed choices about their personal responsibilities within their communities
- it works alongside school and college-based education to encourage young people to achieve and fulfil their potential, and
- it works with other agencies to encourage society to be responsive to young people’s needs. (NYA, 2004: 3)
In his essay on participation written for Unicef, Roger Hart introduced the Ladder of Participation, based on Sherry Arnstein’s 1969 model of citizen involvement in town planning (Hart, 1992). Hart’s ladder describes levels of participation from ‘tokenism’ to ‘citizenship’. He argues that children and young people often experience involvement described as participation but which in reality amounts to ‘decoration’, a kind of window-dressing to make policymakers look responsive and inclusive. Each rung of the ladder represents an improved form of participation, showing children and young people’s growing influence on decision making – until the top rung, where decisions are child and young person-led. Hart was right to make these distinctions and the question ‘Is this real participation?’ is regularly posed both by young people and practitioners.
The ladder has been interrogated for its usefulness over the last two decades and has been adapted to show the efficacy of different kinds of participation in context, thereby removing the judgement implicit in consigning some forms of participation to ‘lower’ rungs. In its participation strategy in 2013, the Office of the Children’s Commissioner for England presented the ‘Wheel of Participation’ (OCC, 2013b) based on Phil Treseder’s work on ‘Degrees of Participation’ for Save the Children in 1997 (itself based on Hart’s ladder). The wheel implies there are different modes of participation suitable for different purposes and no linear approach to using them. Treseder’s work is also referenced by the National Foundation for Educational Research in its ‘Developing Young Researchers’ online guidance 43.
Many researchers have sought to understand the impact of participation both on the individual young people involved and the services they have worked to influence. Fleming (2013) finds cause for both celebration and concern, arguing (as many have before her) that participation works best when young people are social actors with a broad scope of influence on policy and services. However, she notes that even successful participation programmes can often have outcomes that are too narrow: strong on young people developing resilience, confidence and feelings of self-efficacy, but influencing only a small element of a service or policy. Fleming’s argument is that the practice of participation has often fallen short of its promise, leading to a reliance on projects focused on providing young people with the opportunity to give their view of a service or their own care, rather than shaping it directly or profoundly through the lens of their own experience.
Moving on from high-quality participation practice to ‘co-production’
Percy-Smith (quoted in Tisdall, 2008) has argued for a move to ‘collaborative social learning’ that is ‘dialogical and relational’ and away from participation models that are focused on simple input or ‘voice’. Tisdall quotes Percy-Smith:
This is the point at which the highest-quality participation practice, which develops resilience and self-efficacy in young people, merges into what might now be termed ‘co-production’ – bringing young people’s experiences and insights into the foundations of service development and enabling them to develop those services alongside adults. It is apparent from the evidence that there is a tendency for the terms ‘co-production’, ‘co-creation’ or ‘co-design’ to be used interchangeably in the young people’s sector. However, ‘co-production’ is the term that is most usefully defined by the work of Professor Tony Bovaird and others (see below) and can be applied to the high-level participatory work that places young people as service users and ‘experts’ alongside adults (Bovaird and Loeffler, 2012).
A useful example of the bridge between high-quality participation work and co-production of services is found in the work of the What Makes the Difference? project led by Rainer (now Catch22) between 2005 and 2008. (For a full case study see Rainer, 2008.) Project staff worked over a period of months with colleagues in Warwickshire County Council to develop the local authority’s ‘pledge’ to children in care and care leavers, in line with the requirements of Care Matters (DfES, 2007). This involved bringing young people and local authority elected members and officers together to design and agree the pledge. The collaboration went on to inform:
- Establishment of the Children in Care Council and its integration into the council’s democratic structure
- An improved corporate parenting strategy, which reported on progress against the pledge
- Delivery of pan-authority multi-agency training on corporate parenting.
All of this work was developed and delivered with young people as participants and partners and supported by the Director of Children’s Services, who reported its impact to the House of Commons Children, Schools and Families Committee in 2009 44.
A similar process is evident in the work of Young Scot, the national youth information and citizenship charity for 11 to 25-year-olds in Scotland. Young people are involved in high-quality participatory work and their ideas are critical to the development and delivery of services. Not all of their projects involve young people working in partnership with service leaders, but the contribution of the young people is of a high quality.
Young Scot describes its approach to co-design as one that:
- Explore: Uncover issues through gathering insights and genuine experiences from young people.
- Create: Generate ideas and co-create solutions with/by young people.
- Reflect: Consider the future impact and sustainability of the ideas produced.
- Recommend: Produce influential ideas/solutions with young people 45.
Young Scot says it is ‘moving beyond traditional consultation methods’ to support partners to deliver outcomes that are ‘driven by co-design and co-production processes’. It has developed an ‘iterative menu’ of different methods which are ‘holistic, flexible and accessible to suit a variety of strategic impacts and objectives’, from ‘idea jams, Youth Investigation Teams, experience mapping to conversation days and focus groups’.
Young Scot’s case studies show that in most cases, young people are worked with separately and then report, present or discuss their findings with policymakers. This is high-quality participation with good outcomes for young people and good insight for policymakers and service providers, although it does not always include direct collaborative work with adults.
Surrey County Council and FutureGov collaborated on ShiftSurrey, a programme of what they call ‘co-creation’ or ‘co-design’ within the council and its partners to re-imagine and improve services across the council. One of the many projects undertaken during the programme looked at pathway planning for care leavers.
In their article ‘From engagement to co-production: The contribution of users and communities to outcomes and public value’, Bovaird and Loeffler (2012) describe the innovation charity NESTA’s view of co-production:
Bovaird and Loeffler go on to assert that service users are ‘critical success factors’ and ‘know things that many professionals do not know’. Most importantly, they emphasise that service users ‘can engage in collaborative rather than paternalistic relationships with staff, with other service users and with other members of the public’.
It is this collaborative approach between groups that marks out co-production from high-quality participation. In its report By Us, For Us, NESTA describes its co-production process as follows:
They use co-production to:
- Identify opportunities for co-delivered support, taking account of both professional and user perspectives
- Better identify opportunities for recovery and independence
- Focus on the aspirations of service users, breaking down barriers between services and sectors
- Share responsibility for outcomes and a move away from over-dependency on particular services and methods of care
- Facilitate a conversation around the possibilities of experience-based evidence. (NESTA, 2013: 7)
For young people, the experience of being involved in projects that rely on their lived experience and insight to influence the world around them, can be critical to the development of self-efficacy, which in turn is a factor in building personal resilience (Hanson and Holmes, 2014; Research in Practice, 2017). This also applies to young people’s experience of being involved in the decision making that directly affects their lives. The consequence for co-produced models of service development is that young people’s contributions lead to more responsive services and the act of co-production helps to embed participatory practice within services.
Young people and co-production
Government guidance is clear that a young person or child-centered approach to needs assessments is at the heart of effective inter- professional safeguarding of children (HM Government 2015a). Young people themselves have reported that the following are key to effective safeguarding:
- Vigilance: to have adults notice when things are troubling them
- Understanding and action: to understand what is happening; to be heard and understood; and to have that understanding acted upon
- Stability: to be able to develop an on-going stable relationship of trust with those helping them
- Respect: to be treated with the expectation that they are competent rather than not
- Information and engagement: to be informed about and involved in procedures, decisions, concerns and plans
- Explanation: to be informed of the outcome of assessments and decisions and reasons when their views have not met with a positive response
- Support: to be provided with support in their own right as well as a member of their family
- Advocacy: to be provided with advocacy to assist them in putting forward their views. (HM Government 2015a: 11)
Young people have stressed the need for social workers to ‘take them seriously’ and develop a relationship with them over time. This includes having consistent access to the same social worker to avoid the trauma of having to recount stories of abuse repeatedly and to different professionals (Coffey, 2014; Smeaton, 2013b).
Young people can be very able to articulate what they need, given the right support. Young people working with Warrington set out these clear asks of professionals:
- Pay attention: “Notice me and ask me questions.”
- Go at my pace: “Don’t pressure or push, but stick with me.”
- “Don’t judge or blame me.”
- “Let me know you genuinely care.”
- “Focus on my strengths and opportunities as well as risks.”
- “Manage my personal information with care and be honest.”
- “Work with me, not ‘for’ me.”
- “Help me make sense of what’s happened.”
- “Find ways to offer me consistent support.”
- “Think about the ‘whole me’: my other needs and my family and carers.” (Warrington, 2016)
As young people experience greater levels of input into their personal decision making and service development, their resilience grows. Young people who have high levels of resilience brought about through experiences of self-efficacy are more likely to have a positive self-concept, a positive view of their capabilities, better developed problem-solving and self-regulation skills, strong connections with one or more parent or carer, and positive bonds with other pro-social adults and peers (Schofield et al, 2012; Hicks and Stein, 2010).
Peer research projects
Peer research projects have become a popular model of co-production of knowledge, engaging young people in gathering views from their peers and interpreting and presenting data to influence policy or practice. The experience can have enormous benefits for individual young people, developing skills and confidence that helps propel many into further research, higher learning or work (Dixon et al, 2015). It is essential, particularly in the context of sensitive issues such as CSE, that peer research is only undertaken when young people are ready, supported and trained. It may not be appropriate to engage peer researchers in relation to CSE for some areas – but it should not be assumed that peer researchers cannot engage with sensitive issues simply because they are young.
Catch22’s research into the impact of corporate parenting was undertaken by a group of young peer researchers:
‘I am studying health and social care at college and all of these skills I can use in my placements that I work in.' (Dixon et al, 2015: 28 and 141)
The independent evaluation of the peer research reports:
If we list the skills the peer researchers acquired during the study, we find most of the following: administration, organisation, logistics, interpersonal skills, emotional intelligence, relationship building, collaboration and data-handling. Not all of these were taught in the training program! (Dixon et al, 2015: 146)
Reflection pointers
- Are we demonstrating meaningful participatory practice in our CSE services?
- How are we creating opportunities for children, young people and their families to co-produce our services, our policies and our oversight mechanisms?
- How are we supporting the necessary culture shift to ensure the voice of lived experience is treated as a valuable source of knowledge?
- How do local service leaders role-model dialogical learning and co-ownership, in order to support practitioners to do so with children, young people and families?
8. Workforce considerations
This section looks at the evidence relating to some workforce issues, in particular the importance of ensuring high-quality reflective supervision for all professionals working with CSE. It considers the role of supervision in enhancing practice and improving outcomes for children and young people, and also discusses the importance of practitioner resilience both as a factor in workforce retention and as a protective factor for children and young people. It also briefly discusses the concept of ‘practitioner dangerousness’ as a risk factor in CSE work.
8.1 The role of supervision in ensuring a young person-focused service
It is now fourteen years since Lord Laming, in his Inquiry report into the death of Victoria Climbié, made clear that all practitioners working with children should have regular supervision and that social work should be underpinned by regular high-quality reflective supervision in order to promote effective practice (Laming, 2003: Recommendation 45).
In his progress report six years later, Lord Laming went on to emphasise the vital role that high-quality supervision plays in helping to reduce low morale, high levels of stress and workforce attrition.
That same year, however, Hunter (2009) reported the ‘sporadic nature’ of supervision across the country and suggested little had changed since 2003. Eight years on, there is evidence to suggest things are improving, with a number of examples cited in the Department for Education’s 2014 document Rethinking Children’s Social Work, which outlined the aims of the Children’s Social Care Innovation Programme.
The role of supervision in supporting professional judgement is well documented (Munro 2011; Ofsted, 2010). It is highlighted as an essential means of developing practice rather than simply ‘checking’ whether work has been carried out. For example, the Department for Education notes the importance of the developmental function of supervision:
High-quality reflective supervision enhances practice and can potentially play a role in improving outcomes for children and young people (Morrison, 2001; 2005) though it is very difficult to trace a direct link from supervision to individual outcomes (Earle et al, 2017). Supervision has been found to help avoid drift, maintain focus on the child, ensure objectivity, interrogate and test the evidence base for assessment and plans, and address the emotional impact of the work (Fox, 2011; Earle et al, 2017) all of which are key.
High-quality, reflective supervision which provides space and time to discuss the wellbeing and impact of the work on the professional, will contribute indirectly to better services for children, provided by staff members who feel empowered, feel a sense of mastery and are supported to develop a sense of emotional resilience. This last point is particularly significant as evidence shows that promoting resilience among practitioners is an organisation-wide responsibility (Grant and Kinman, 2016); ensuring supervision is fit for purpose is one of the key things local leaders can do to support practitioner resilience.
Supervision and CSE
Every professional should have access to a supervisor with whom they can talk through their concerns and judgements affecting the welfare of a young person at risk of, or who has experienced, sexual exploitation. Existing literature locates supervision within safeguarding and child protection generally; CSE work is part of safeguarding and therefore those principles apply. However, there are specific nuances that supervision within the context of CSE work needs to address. These include ensuring practitioners understand what CSE is and, in particular, developing practitioners’ understanding of adolescent development, agency and choice, hidden harm, and the underlying reasons for particular behaviours shown by children experiencing trauma. Supervision also needs to support practitioners to work within the unpredictable and complex context of CSE and the multiple, dynamic and inter-related factors that affect a child or young person’s life, any one of which can influence their situation.
Although there are different approaches and models for supervision, there is no one identified model that can be recommended above others for use within the context of CSE. Whichever model is applied, supervisors need to ensure they incorporate the four functions of accountability, development, support and mediation (Fox, 2011). Safeguarding supervision should combine critical reflective practice and critical thinking with a restorative experience so that the professional feels supported and is able to maintain their capacity to think (Earle et al, 2017; Morrison, 2005; Wonnacott, 2012). Wallbank and Wonnacott (2015) urge that individuals undertaking safeguarding supervision are appropriately trained to identify how they can support other professionals to retain their reflective capacity and decision-making skills.
Fox (2011) usefully draws on the work of Morrison (2001; 2005) and provides an overview of effective supervision and models. For a more detailed discussion and practical tools to support reflective supervision, see Research in Practice’s ‘Reflective Supervision: Resource Pack’ (Earle et al, 2017), which is aimed at staff with supervisory responsibilities. It includes activities, worksheets and frameworks to promote group supervision, audits, critical thinking and analysis, emotional resilience and recording 46.
8.2 Supervision and assessment
Whilst it is important to understand CSE, identify it and understand and own our feelings about it as a social phenomenon, it is the assessment that will ensure the right help gets to the young person at the right time. Supervision must support professionals to make good-quality and evidence-informed decisions, based on analysis, judgement and professional knowledge. In their thematic inspection, The Quality of Assessment for Children in Need of Help, Ofsted (2015) link effective supervision involving developmental support to improved quality of assessment. Ofsted found that in high-performing local authorities, leaders ensured there was robust, reflective managerial supervision and oversight of practitioners carrying out assessments. These local authorities prioritised supportive supervision (including group supervision) as a means of developing assessment practice.
Given that CSE requires professionals across agencies to be able to recognise risks and assess needs in order to construct a holistic view of a young person, it is important that supervision is not restricted to social work. Those working with young people in other disciplines must also be able to access high-quality supervision, not least because it will support them in their assessment practice. There is relatively little research regarding supervision among the youth work profession, but in 2013 an Ofsted good practice case study (‘Effective professional development in youth services’ – Bath and North East Somerset Council) demonstrated the significance of supervision in enabling reflective practice and in developing practitioners’ knowledge of working with particularly marginalised groups.
Reflection pointers
- How confident are we that professionals across disciplines have access to the high-quality reflective supervision that is needed to support good decision making with, and for, young people affected by CSE?
- How do we evaluate the impact of supervision practice on the quality of assessments, on the quality of plans, on practitioners’ knowledge, and on team and service culture?
- What role might a specialist CSE service play in building capacity for reflective supervision in other agencies?
- How do we support those carrying out supervision to develop their skills and confidence, so that supervision is of a consistently high quality?
8.3 Emotional impact of CSE, supervision and staff resilience
While social workers and other practitioners may successfully promote resilience in the client group they work with, they may pay less attention to, or be less aware of, their own needs and how to develop their resilience (Laming, 2009; Research in Practice, 2014c). It is worth noting here that Kinman and Grant (2011) found a significant negative relationship between resilience and psychological distress in UK social work trainees; individuals with more developed emotional and social competencies, including reflective ability, were more resilient to stress. Research by Ben-Porat and Itzhaky (2015) found it was new workers and the most experienced workers who were most likely to experience vicarious trauma (and burnout) in cases of CSA and so may need extra/enhanced supervision.
A study by Conrad and Kellar-Guenther (2006) found that around half of all social workers had experienced their own trauma and a meta-analysis of therapists working in this field showed that therapists exhibited the same trauma symptoms as the people they were helping (Figley, 1995). This is important to consider, since the findings from Ben-Porat and Itzhaky (2015) showed that past exposure to trauma contributed significantly to workers’ levels of vicarious trauma and burnout. Other significant factors were the worker’s age, experience, sense of mastery in their role, self-esteem and influence in the workplace. Applications of this study include the conclusion that burnout can be reduced when: staff have access to clinical supervision that focuses on their wellbeing; staff are effectively debriefed after each distressing incident or disclosure; and staff feel a sense of influence or mastery in the workplace, including over the procedures followed and decisions taken in relation to their cases and work environment. These findings are supported by NSPCC (2013c).
Staff training and support, including a focus on building resilience, are also crucial to staff retention (Research in Practice, 2014c; Grant and Kinman, 2016). High staff turnover in the social work sector is placing pressure on current staff; nearly half of local councils experienced challenges in staff retention in 2012-13 (Wiseman and Davies, 2013). The child protection literature suggests supervision may play an important role in staff retention. Gibbs (2001) suggests supervision can lower attrition rates among child protection workers and this may prove to be true of other emotionally demanding roles in the context of CSE.
Reflection pointers
- How confident are we that professionals across all partner agencies are supported to develop their resilience and manage the emotional impact of working with CSE?
- How do we ensure that professionals are able to recognise stressors and risk of burnout? How do we know whether the support in place is effective?
- Do local leaders demonstrate an understanding of the emotional impact of the work on those dealing directly with CSE? How do local service leaders and policies enable, or impede, professionals’ sense of mastery / self-efficacy?
Practitioner (or organisational) dangerousness as a risk factor
The concept of ‘practitioner dangerousness’ within child protection research emerged in light of situations where there had been ‘failures’ to effectively protect children from abuse within the home (Crighton, 2005). It occurs when inappropriate values, priorities or methods lead practitioners to act in ways that fail to reduce the risk to children and young people, thereby leaving them in a vulnerable situation that could potentially increase risk. Whilst this concept emerged specifically in relation to intra-familial child abuse within the home, there are some transferable issues that practitioners and mangers working in the context of CSE should be aware of. These include: inadequate supervision and high caseloads (making it hard for practitioners to reflect and hypothesise); technology-driven practice that focuses on documentation rather than spending time with children and young people; and a lack of focus on the child or young person (with other issues distracting attention). In designing or refining new or existing CSE services, it may be helpful to consider how the design takes account of these potential pitfalls.
Key messages
- Practitioners in the field of CSE are, of course, all humans with personal histories and are likely to be impacted by the work they do. Burnout and vicarious trauma is common and needs to be perceived as a real trauma rather than just ‘part of the job’.
- High quality clinical supervision, debriefing, and empowering practitioners to have a sense of mastery and influence over their cases and workplace, can all help reduce burnout.
- Reflective supervision is vital. It enhances practice and so can help to improve outcomes. It can help avoid drift, maintain objectivity and maintain focus on the child. It can help test the evidence base for assessment and plans, and address the emotional impact of the work.
- There are specific nuances that supervision within the context of CSE work needs to address. These include understanding what CSE is and, in particular, understandings of adolescent development, agency and choice, hidden harm and the reasons for young people’s behaviour or responses.
- Reflective supervision can help develop and maintain practitioner resilience. Practitioners with more developed emotional and social competencies, including reflective ability, are likely to be more resilient to stress.
- Enabling practitioners to build strong and enduring relationships with young people is critical to addressing CSE effectively, which is of course dependent on workforce stability. Supervision and staff training are linked to staff retention and therefore a vital factor in ensuring sustained relationships are provided to children and young people affected by CSE.
- A lack of focus on the individual needs of a child or young person is a key theme in practitioner or organisational ‘dangerousness’. Reflective practice and supervision is one way of avoiding this.
9. Six key principles for service design and practice development
Drawing on the body of evidence within this scope, six key principles are identified as being central to understanding and addressing CSE effectively. These are intended to inform the development or redesign of CSE services and to support good practice.
- Young people must be at the centre and should not be held responsible for their harm or their safety.
- CSE is complex; therefore the response cannot be simple or linear. Responses need to be based on evidence from a wide range of sources of expertise.
- No agency can address CSE in isolation; collaboration is essential.
- Knowledge is crucial.
- Communities and families are valuable assets, and are likely to need support.
- Effective services require resilient and supported practitioners.
Table 9.1 expands these principles, with examples of how each principle would look in practice.
Table 9.1 (as follows): Six key principles for service design and practice development
1. Children and young people must be at the centre
- Children and young people are listened to, respected and included in service design and evaluation; their expertise is used to continuously improve service delivery.
- At individual practice level, children and young people are involved in decisions made about them and are enabled to take ownership of the change process; workers are supported to navigate the complexities of participatory practice.
- Practitioners do not label or define a child or young person by their behaviour and do not imply or apportion blame to young victims, but recognise that particular behaviours or responses may be a coping strategy or (mal)adaption to previous harm.
- Assessments are needs led, using frameworks and approaches that elicit the particular needs and circumstances of individual children and young people, rather than using rigid or linear models. Strengths and resilience factors are also explored within assessment.
- Services and pathways between services are designed with children and young people in mind and reflect the specific needs, strengths and vulnerabilities of these groups.
- Relationships can transform lives; a child or young person should be an active agent in this therapeutic relationship rather than the passive recipient of a service.
- Children and young people should receive comprehensive education about sex, abuse and relationships but this should not be used as a preventative method, and care must be taken to avoid re-traumatising victims when using educational resources.
2. CSE is complex; therefore the response cannot be simple or linear
- The methods and approaches employed to groom and exploit children are varied, and often co-exist; strategy and service design must reflect this complexity.
- Assessment tools are evidence-informed without being overly rigid; assessment practice demonstrates an understanding of the multiple dynamic factors and how they inter-relate.
- Service design and processes reflect the complexity of CSE, its pathways and impacts and therefore do not prescribe a one- size-fits-all response for children and young people.
- Commissioning and planning activity recognises that service responses may need to be long term, particularly for those left traumatised by the harm they have experienced, and that referral pathways need to be fluid.
- Practitioners are appropriately trained and supported to understand and work within the complex dynamics of CSE.
- Dual identities are recognised in individual practice and service-level responses – e.g., victims of CSE may also be identified as perpetrators, parents may be both a source of conflict and protection.
3. No agency can address CSE in isolation; collaboration is essential
- Safeguarding is promoted and accepted as being the responsibility of all those who come into contact with children and young people, and professional groups are clear on the unique contribution they make to the to the whole system.
- Strategic initiatives draw on the expertise held by different agencies, and efforts are made to align priorities and resources; multi-agency collaboration is enabled by shared goals, shared language and shared values as well as shared practice tools.
- Universal services understand their role in providing preventative interventions and are equipped and supported to do so.
- Schools and other community-based settings are actively engaged in promoting excellent RSE and building children and young people’s understanding of sex, abuse and relationships and in challenging cultural attitudes that can facilitate exploitation.
- Specialist services are adequately resourced to provide targeted interventions for children and young people affected by CSE; they are a source of knowledge and expertise to other services rather than operating separately or in isolation.
- Hierarchies between professional groups are recognised and managed by local leaders in order to ensure that the strengths and contribution of each agency are facilitated.
- Information sharing is critical, both at practitioner and service level; protocols should be reviewed at regular intervals and feedback from practitioners about barriers to information sharing should be used to improve process and strategy.
4. Knowledge is crucial
- Knowledge must be kept up to date, as research and practice wisdom evolves. Established practices should never act as a barrier to incorporating new knowledge.
- Practitioners and managers across agencies understand contemporary conceptualisations of CSE and are familiar with local and national policy definitions and methods.
- Children and young people have knowledge of CSE, are able to recognise CSE and understand the nature of healthy relationships. Communities understand what CSE is and what to do if it is identified.
- Local data is used to identify local needs and service requirements for both universal and specialist services. Commissioning is based on high-quality needs data. Community intelligence is used, where appropriate, to inform local needs analysis.
- Practitioners and managers across agencies understand the current evidence and arguments surrounding indicators and risk factors for CSE and take responsibility for ensuring that families, professionals and communities also have the knowledge they require to identify when CSE may be occurring.
- Information is provided to families, in a way that is accessible and non-judgmental, in order to build their knowledge.
- Practitioners across agencies have access to high-quality learning and development opportunities; knowledge sharing is enabled between agencies; and specialist services support non-specialist services to build their knowledge, skills and confidence.
- Practitioners are trained to understand, identify and challenge victim blaming and stereotyping of victims of CSE.
5. Communities and families are valuable assets, and are likely to need support
- The wider community is supported to understand their role in protecting children and young people from harm.
- Communities are engaged in intelligence gathering and ‘problem profiling’ activity to inform local needs analysis, but also acknowledge that CSE is not a geographically situated crime and communities should always assume CSE could be occuring.
- Clear information is available to communities so that they can recognise CSE and act accordingly, and feedback is sought to ensure this is working effectively.
- The protective role that families can play in addressing CSE is recognised in the way services are constructed as well as at individual case level.
- The possibility of CSE victims having experienced previous trauma, including early harm within the family, is recognised and explored – but not assumed – by practitioners.
- Families are supported to engage with CSE work for their child and are, wherever possible and appropriate, treated as key players in the team around the child.
- Positive relationships between young people at risk of, or experiencing, CSE and their families are actively promoted by the professionals working with them, wherever possible and appropriate.
6. Effective services require resilient and supported practitioners
- The emotional impact of CSE work on practitioners is recognised by service leaders, and this understanding is reflected in strategy, policy and leadership practice.
- Practitioners across agencies receive high-quality reflective supervision which supports them to develop critical thinking skills, assessment skills and promotes their resilience.
- Attention is paid to the impact of CSE work when allocating cases, structuring services and planning staff recruitment and retention activity.
- Service leaders proactively create a culture where resilience is promoted across the workforce, and are alert to the practice pitfalls, poor judgement and ‘blind spots’ (which can emerge in part due to diminished practitioner resilience).
- High-quality learning and development opportunities are provided for those working with young people at risk of, or experiencing, CSE, which go beyond formal training to include structured peer support, group supervision and involvement in service development.
- The quality and impact of supervision and of learning and development is evaluated.
Footnotes
-
Although younger children may be under-identified as victims of CSE
-
A parallel exercise was undertaken to engage and learn from children and young people, as part of the overall project.
-
The government’s statutory guidance Working Together to Safeguard Children (HM Government 2015a) was updated in February 2017 to include the revised definition.
-
Child sexual exploitation: Practice Tool. Research in Practice
-
See NSPCC’s ‘Sexual abuse: facts and statistics
-
Information provided by Barnardo’s September 2017
-
See the government’s response (May 2016) to the Wood Review of LSCBs
-
Operation Striver is a set of information forms and protocols to collect information about CSE concerns from professionals and agencies in certain police force areas, in order to collate data and intelligence about potential sex offenders and victims that may have been moving across force and local authority areas. Information is submitted on a form and then collected and analysed by the police to look for trends, themes and patterns.
-
See the College of Policing’s online guidance ‘Responding to child sexual exploitation’
-
Operation Retriever occurred in Derby and led to the conviction of 13 men for the sexual exploitation of children. Operation Kern occurred in Derby shortly afterwards; eight men were convicted of sexual exploitation of children. Operation Retriever has double the amount of search engine results than Kern, was reported by national news outlets (including the BBC and The Guardian) and features in almost all LSCB CSE strategies in England as an example of a CSE case that was prosecuted. Operation Kern, on the other hand, received little to no national press coverage, despite being heavily covered by local media outlets.
-
A sex offender is someone who commits a sexual offence. A paedophile is defined as a person with a sexual preference for pre- pubescent children (DSM-V). Therefore, the majority of offenders convicted in CSE cases are/were not paedophiles.
-
'Almost 9 out of 10 parents think children are being forced to grow up too quickly', 11 April 2011
-
s.34 of the Children and Social Work Act uses the wording 'relationships and sex education'; organisations and educators often use ‘sex and relationships education (SRE)’.
-
In March 2017 the government announced its intention that pupils would be taught the new curriculum from September 2019, following public consultation on draft regulations and statutory guidance.
-
Information provided by Barnardo’s October 2017
-
Note: Whilst the LGA guidance states that ‘any child under 18 cannot consent to being trafficked for the purposes of exploitation’ it is worth noting that this is also true for adults. No one can ‘consent’ to being trafficked and sexually exploited.
-
UK poll for Amnesty International, press release 21 November 2005
-
ACT is the CSE service emerging from the Wigan and Rochdale Innovation Project within which this scope was originally commissioned.
-
Information provided by managers overseeing the ACT service October 2017
-
See the College of Policing's online guidance 'Responding to child sexual exploitation'
-
See also Blue Knot’s online guidance ‘Best practice guidelines for working with adults surviving child abuse’
-
See www.barnardos.org.uk/get_involved/campaign/cse/spotthesigns.htm
-
Information provided by managers working within Project Phoenix October 2017
-
Information provided by managers overseeing ACT project, October 2017
-
See NSPCC evaluation reports for GCP and GCP2 (now offline)
-
www.nwgnetwork.org/events/cse-aThissessment-launch (now offline)
-
For information on the Sexual Behaviours Traffic Light Tool.
-
The methodology supporting the analysis from HMT (now offline)
-
London sexual exploitation operating protocol (3rd edition)
-
YouGov Poll Exposes High Levels Sexual Harassment in Schools
-
Borderline personality disorder or BPD is the centre of considerable debate and controversy due to its labelling and framing of a person’s behaviour and difficulties as evidence of a disordered personality, rather than a legitimate response to cumulative trauma. Use of the term here does not imply uncritical acceptance.
-
For more information on Project Phoenix.
-
www.nfer.ac.uk/schools/developing-young-researchers/involving-young-people.cfm (now offline)
-
www.youngscot.net/what-we-do/co-design-service and www.youngscot.net/wp-content/uploads/2015/02/Co-design-Offer.pdf (now offline)
-
Research in Practice: Practice tools and guides
References
Abel K et al (2012) The WEMSS Report: A clinical, economic and operational evaluation of the pilot for Women’s Enhanced Medium Secure Services (WEMSS) Informing Secure Pathways for Women. London: HMSO.
Alfoadari K and Anderson C (undated) ‘Oxfordshire Looked After Children Dialectical Behavioural Therapy (DBT) Service’ (Presentation slides.) Oxfordshire and Buckinghamshire Mental Health Partnership NHS Trust.
Allnock D (2016) Exploring the Relationship between Neglect and Adult-perpetrated Intra-familial Child Sexual Abuse: An evidence scope. Dartington: Action for Children, NSPCC and Research in Practice.
Allnock D and Hynes P (2012) Therapeutic Services for Sexually Abused Children and Young People: Scoping the evidence base. London: NSPCC.
Allnock D and Miller P (2013) No One Noticed, No One Heard: A study of disclosures of childhood abuse. London: NSPCC.
American Psychological Association (2007) Report of the APA Taskforce on the Sexualization of Girls. Washington, DC: APA.
Anderson I, Beattie G and Spencer C (2001) ‘Can blaming victims be logical? Attribution theory and discourse analytic perspectives’, Human Relations, 54 (4) 445-467.
Attwood F (2006) ‘Sexed up: Theorizing the sexualization of culture’, Sexualities, 9 (1) 77-94.
Baginsky M and Holmes D (2015) A Review of Current Arrangements for the Operation of Local Safeguarding Children Boards. Dartington: Research in Practice.
Bailey R (2011) Letting Children be Children: Report of an Independent Review of the Commercialisation and Sexualisation of Childhood. London: Department for Education.
Barlow J and Scott J (2010) Safeguarding in the 21st Century – Where to Now? Dartington: Research in Practice.
Barlow J, Fisher J and Jones D (2012) Systematic Review of Models of Analysing Significant Harm. London: Department for Education.
Barnardo’s (2007a) Sexual Exploitation Risk Assessment Framework. A pilot study. London: Barnardo’s.
Barnardo’s (2007b) Bwise2 Sexual Exploitation: A preventative education pack for use with 12 to 17-year-olds in pupil referral units, residential units and schools – England and Wales edition. London: Barnardo’s.
Barnardo’s (2011a) Puppet on a String: The urgent need to cut children free from sexual exploitation. Ilford: Barnardo’s.
Barnardo’s (2011b) Reducing the Risk, Cutting the Cost: An assessment of the potential savings on Barnardo’s interventions for young people who have been sexually exploited. Ilford: Barnardo’s.
Barnardo’s (2014a) Hidden in Plain Sight. A scoping study into the sexual exploitation of boys and young men in the UK. Ilford: Barnardo’s.
Barnardo’s (2014b) Report of the Parliamentary Inquiry into the Effectiveness of Legislation for Tackling Child Sexual Exploitation and Trafficking within the UK. Chaired by Sarah Champion. Ilford: Barnardo’s.
Barnardo’s (2017) Working with Children who are Victims or at Risk of Sexual Exploitation: Barnardo’s model of practice. Ilford: Barnardo’s.
Barnardo’s and the Local Government Association (2012) Tackling Child Sexual Exploitation: Helping local authorities to develop effective responses. Ilford: Barnardo’s.
Barrett D, Barrett E and Mullenger N (2000) Youth Prostitution in the New Europe: The growth of sex work. Lyme Regis: Russell House Publishing.
Barter C, McCarry M, Berridge D and Evans K (2009) Partner Exploitation and Violence in Teenage Intimate Relationships. NSPCC.
Beckett H (2011a) Not a World Away: The sexual exploitation of children and young people in Northern Ireland. Belfast: Barnardo’s NI.
Beckett H (2011b) 10 Key facts about child sexual exploitation. (Research Briefing Note #1 produced to support a short film for practice). Luton: University of Bedfordshire. (film)
Beckett H and Walker J (forthcoming Jan 2018) ‘Words matter: Reconceptualising the conceptualisation of child sexual exploitation’, in Beckett H and Pearce J (eds) Understanding and Responding to Child Sexual Exploitation. London: Routledge.
Beckett H and Warrington C (2015) Making Justice Work: Experiences of criminal justice for children and young people affected by sexual exploitation as victims and witnesses. Luton: University of Bedfordshire.
Beckett H, Holmes D and Walker J (2017) Child Sexual Exploitation: Definition and guide for professionals. (Extended text). Luton: University of Bedfordshire, Research in Practice.
Bedford A (2015) Serious Case Review into Child Sexual Exploitation in Oxfordshire: from the experiences of Children A, B, C, D, E, and F. Oxford: Oxfordshire Safeguarding Children Board.
Beech A, Elliott I, Birgden A and Findlater D (2008) ‘The Internet and child sexual offending: A criminological review’, Aggression and Violent Behavior, 13 (3) 216-228.
Ben-Porat A and Itzhaky H (2015) ‘Burnout among trauma social workers: The contribution of personal and environmental resources’, Journal of Social Work, 15 (6) 606-620.
Berridge D, Biehal N and Henry L (2012) Living in Children’s Residential Homes. London: Department for Education.
Bilston B (2006) ‘A history of child protection’, Article published on the Open University Open Learn website.
Blue Knot Foundation (2017) Practice Guidelines for Treatment of Complex Trauma and Trauma Informed Care and Service Delivery. Milson’s Point, NSW: Blue Knot Foundation.
Boer D (ed) (2016) The Wiley Handbook of Theories, Assessment and Treatment of Sexual Offending: Volume III Treatment. John Wiley and Sons.
Bovaird T and Loeffler E (2012) ‘From engagement to co-production: The contribution of users and communities to outcomes and public value’, Voluntas: International Journal Of Voluntary and Non-profit Organizations, 23 (4) 1119-11 38.
Bovarnick S and Scott S (2016) Child Sexual Exploitation Prevention Education: A rapid evidence assessment. Luton: Barnardo’s and University of Bedfordshire.
Bradford S (2004) ‘Management of growing up’, in Roche J, Tucker S, Thomson R and Flynn R (eds), Youth in Society: Contemporary Theory, Policy and Practice. Second Edition. London: Sage/Open University.
Bradley A and Wood J (1996) ‘How do children tell? The disclosure process in child sexual abuse’, Child Abuse & Neglect, 20 (9) 881-891.
Brandon M, Bailey S, Belderson P, Gardner R, Sidebotham P and Dodsworth J (2009) Understanding Serious Case Reviews and their Impact: A Biennial Analysis of Serious Case Reviews 2005-07. London: Department for Children, Schools and Families.
Brandon M, Bailey S and Belderson P (2010) Building on the Learning from Serious Case Reviews: A two-year analysis of child protection database notifications 2007-2009. Department for Education.
Brandon M, Sidebotham P, Bailey S, Belderson P, Hawley C, Ellis C and Megson M (2012) New Learning from Serious Case Reviews. London: Department for Education.
Brayley H and Cockbain E (2012) ‘Group-based child sexual exploitation (1-Summary’, (JDiBrief series of briefing notes). London: University College London, Jill Dando Institute of Security and Crime Science.
Breckon J and Hay J (2015) Knowing How to Protect: Using research and evidence to prevent harm to children. London: Alliance for Useful Evidence and NSPCC.
Brodie I, Melrose M, Pearce J and Warrington C (2011) Providing Safe and Supported Accommodation for Young People who are in the Care System and who are at Risk of, or Experiencing, Sexual Exploitation or Trafficking for Sexual Exploitation. University of Bedfordshire / NSPCC.
Brodie I with D’Arcy K, Harris J, Roker D, Shuker L and Pearce J (2016) The Participation of Young People in Child Sexual Exploitation Services: A scoping review of the literature. Luton: University of Bedfordshire.
Bronfenbrenner U (1979) The Ecology of Human Development: Experiments by nature and design. Cambridge, MA: Harvard University Press.
Brook, PSHE Association and Sex Education Forum (2014) Sex and Relationships Education (SRE) for the 21st century. Supplementary advice to the ‘Sex and Relationship Education Guidance’ DFEE (0116/2000). Brook, PSHE Association and Sex Education Forum.
Brooks C and Brocklehurst P (2014) Safeguarding Pressures Phase 4, November 2014. Manchester: ADCS.
Brown H, Sebba J and Luke N (2014) The Role of the Supervising Social Worker in Foster Care: An international literature review. Oxford: Rees Centre for Research in Fostering and Education, University of Oxford.
Brown R and Ward H (2013) Decision-making within a Child’s Timeframe: An overview of current research evidence for family justice professionals concerning child development and the impact of maltreatment. London: Childhood Well-being Research Centre.
Brown S (2005) Understanding Youth and Crime, Buckingham: Open University Press.
Brown S, Brady G, Franklin A, Bradley L, Kerrigan N and Sealey C (2016) Child Sexual Abuse and Exploitation: Understanding risk and vulnerability. London: Early Intervention Foundation.
Brown S, Brady G, Franklin A, and Crookes R (2017 forthcoming) Exploratory study on the use of tools and checklists to assess risk of child sexual exploitation. Centre of Expertise on Child Sexual Abuse.
Burge T (1986) ‘Individualism and psychology’, The Philosophical Review, 95 (1) 3-45.
Burman M and Batchelor S (2009) ‘Between two stools? Responding to young women who offend’, Youth Justice, 9 (3) 270-285.
Bywaters P, Featherstone B, Morris K, Daniel B, Brady G, Bunting L, Mason W and Mirza N (2017) ‘Poverty, inequality, child abuse and neglect: Changing the conversation across the UK in child protection?’, Children and Youth Services Review, DOI: 10.1016/j. childyouth.2017.06.009.
The Care Inquiry (2013) Making Not Breaking: Building relationships for our most vulnerable children. Findings and recommendations of the Care Inquiry.
Casey L (2015) Report of Inspection of Rotherham Metropolitan Borough Council. Great Britain. London: Department for Communities and Local Government.
CEOP (2007) ‘UK dedicated centre for tackling child sex abuse launches online safety programme for 8-11 year olds’, CEOP Command press release.
CEOP (2013) Threat Assessment of Child Sexual Exploitation and Abuse. London: Child Exploitation and Online Protection Centre.
Chase E and Statham J (2005) ‘Commercial sexual exploitation of children and young people in the UK – a review’, Child Abuse Review, 14 (1) 4-25.
Chen E, Shofer F, Dean A, Hollander J, Baxt W, Robey J et al (2008) ‘Gender disparity in analgesic treatment of emergency department patients with acute abdominal pain’, Academic Emergency Medicine, 15 (5) 414-8, DOI: 10.1111/j.1553-2712.2008.00100.x
Chen L, Murad M, Paras M, Colbenson K, Sattler A, Goranson E, Elamin M, Seime R, Shinozaki G, Prokop L and Zirakzadeh A (2010) ‘Sexual abuse and lifetime diagnosis of psychiatric disorders: Systematic review and meta-analysis’, Mayo Clinic Proceedings, 85 (7) 618-629, DOI: 10.4065/mcp.2009.0583.
Chief Medical Officer (2013) Our Children Deserve Better: Prevention pays. Annual report of the Chief Medical Officer 2012.
Children and Social Work Act 2017
Children’s Society (2013) Standing Tall After Feeling Small
Children’s Society (2014) What is child sexual exploitation? Children’s Society.
Child Welfare Information Gateway (2009) Child Maltreatment. Washington DC: Children’s Bureau. Clutton S and Coles J (2008) Child Sexual Exploitation in Wales: 3 years on. Cardiff: Barnardo’s Cymru.
Cockbain E, Brayley H and Ashby M (2014) Not Just a Girl Thing: A large-scale comparison of male and female users of child sexual exploitation services in the UK. Ilford: Barnardo’s.
Cockbain E, Ashby M and Brayley H (2015) ‘Immaterial boys? A large-scale exploration of gender-based differences in child sexual exploitation service users’, Sexual Abuse: A Journal of Research and Treatment, doi.org/10.1177/1079063215616817
Coffey A (2014) Real Voices: Child sexual exploitation in Greater Manchester. An independent report by Ann Coffey MP.
Coleman J and Hagell A (eds) (2007) Adolescence, Risk and Resilience: Against the odds. Chichester: Wiley.
College of Policing ‘Responding to child sexual exploitation’. Online guidance.
Conrad D and Kellar-Guenther (2006) ‘Compassion fatigue, burnout and compassion satisfaction among Colorado child protection workers’, Child Abuse and Neglect, 30 (10) 1071-1080.
Corby B (2006) Child Abuse: Towards a knowledge base. Maidenhead: Open University Press.
Council of Europe (2012) Recommendation on the Participation of Children and Young People under the age of 18. Strasbourg: Council of Europe.
Coveney P and Highfield R (1996) Frontiers of Complexity: The search for order in a chaotic world. London: Faber and Faber.
Coy M (2008) ‘Young women, local authority care and selling sex: Findings from research’, British Journal of Social Work, 38 (7) 1408- 1424.
Coy M, Sharp-Jeffs N and Kelly L (2017) Key Messages from Research on Child Sexual Exploitation: Strategic commissioning of children’s services. London: London Metropolitan University, Child & Woman Abuse Studies Unit.
Craven S, Brown S and Gilchrist E (2006) ‘Sexual grooming of children: Review of literature and theoretical considerations’, Journal of Sexual Aggression, 12 (3) 287–299.
Creegan C, Scott S and Smith R (2005) The Use of Secure Accommodation and Alternative Provisions for Sexually Exploited Young People in Scotland. Ilford: Barnardo’s
Cretser G, Lombardo W, Lombardo B and Mathis S (1982) ‘Reactions to men and women who cry: A study of sex differences in perceived societal attitudes versus personal attitudes’, Perceptual and Motor Skills, 55 (2) 479-486.
Crighton D (2005) ‘Risk assessment’, in Crighton D and Towl G (eds) Psychology in Probation Services. Oxford: BPS Blackwell.
D’Andrade A, Benton A and Austin M J (2005) Risk and Safety Assessment in Child Welfare: Instrument comparison. Berkeley: Bay Area Social Services Consortium.
D’Andrade A, Austin M J and Benton A (2008) ‘Risk and safety assessment in child welfare: instrument comparisons’, Journal of Evidence Based Social Work, 5 (1-2) 31-56.
Daniel B (2010) ‘Concepts of adversity, risk, vulnerability and resilience: A discussion in the context of the “Child Protection System”’, Social Policy and Society, 9 (2) 231-241.
Daniel B, Burgess C and Scott J (2012) Review of Child Neglect in Scotland. The Scottish Government.
D’Arcy K and Thomas R (2016) Nightwatch: CSE in Plain Sight. Final evaluation report. Luton: University of Bedforshire.
D’Arcy K, Dhaliwal S, Thomas R, Brodie I and Pearce J (2015) Families and Communities Against Child Sexual Exploitation (FCASE): Final evaluation report. Luton: University of Bedfordshire.
Davies B (1996) ‘At your service?’ Young People Now, August, pp26-27.
Department for Children, Schools and Families (2007) The Children’s Plan: Building brighter futures. London: DCSF.
Department for Children, Schools and Families (2009) Safeguarding Children and Young People from Sexual Exploitation. HMSO: London.
Department for Education (2011) UK Resilience Programme Evaluation: Final Report. London: DfE. Department for Education (2012) Tackling Child Sexual Exploitation Action Plan: Progress report. London: DfE.
Department for Education (2014) Rethinking Children’s Social Work. Department for Education’s Children’s Social Care Innovation Programme. London: DfE.
Department for Education (2017) Child Sexual Exploitation: Definition and a guide for practitioners, local leaders and decision makers. London: DfE.
Department for Education and Skills (2007) Care Matters: Time for change. London: DfES.
Department of Health (2014) Health Working Group Report on Child Sexual Exploitation. London: DH.
Department of Health and Public Health England (2015) School Nurse Programme: Supporting the implementation of the new service offer: Helping school nurses to tackle child sexual exploitation. London: DH.
Department of Health, Department for Education and Employment, and Home Office (2000) Framework for the Assessment of Children in Need and Their Families. London: The Stationery Office.
DePrince A (2005) ‘Social cognition and revictimization risk’, Journal of Trauma and Dissociation, 6 (1) 125-141.
DePrince A, Brown L, Cheir R, Freyd J, Gold S, Pezdek and Quina K (2012) ‘Motivated forgetting and misremembering: Perspectives from betrayal trauma theory’, in Belli R (ed) True and False Recovered Memories: Toward a reconciliation of the debate (Nebraska Symposium on Motivation 58). London: Springer.
Dixon J and Lee J, with Stein M, Guhirwa H, Bowley S and Catch 22 Peer Researchers (2015) Corporate Parenting for Young People in Care: Making the difference?
Dodsworth (2014) ‘Sexual exploitation, selling and swapping sex: Victimhood and agency’, Child Abuse Review, 23 (3) 185-199.
Doherr L, Reynolds S, Wetherly J and Evans E (2005) ‘Young children’s ability to engage in cognitive therapy tasks: Associations with age and educational experience’, Behavioural and Cognitive Psychotherapy, 33 (2) 201-215.
Dorsey S, Mustillo S, Farmer E and Elbogen E (2008) ‘Caseworker assessments of risk for recurrent maltreatment: Association with case-specific risk factors and re-reports’, Child Abuse Neglect, 32 (3) 377–391.
Earle F, Fox J, Webb C and Bowyer S (2017) Reflective Supervision: Resource Pack. Dartington: Research in Practice.
Eaton J (forthcoming) ‘Things she should have done differently: Exploring the factors related to the victim blaming of women and girls affected by sexual violence’, University of Birmingham.
Elliott M (1995) ‘Child sexual abuse prevention: What offenders tell us’, Child Abuse and Neglect, 19 (5) 579-594.
End Violence Against Women (2011) A Different World is Possible: A call for long-term and targeted action to prevent violence against women and girls. Published by the EVAW Coalition.
Ericson R and Doyle A (2005) Risk and Morality. Toronto: University of Toronto Press.
European Online Grooming Project (2012) Final Report. (Report prepared for the European Commission Safer Internet Plus Programme.)
Family Planning Queensland (now True) (2012) Traffic Lights Guide to Sexual Behaviours in Children and Young People: Identify, understand and respond. Brisbane: Family Planning Queensland, Australia.
Fargion S (2014) ‘Synergies and tensions in child protection and parent support: Policy lines and practitioners cultures’, Child & Family Social Work, 19 (1) 24-33.
Farmer E and Pollock S (1998) Sexually Abused and Abusing Children in Substitute Care. Chichester: Wiley.
Featherstone B, White S and Morris K (2014) Re-imagining Child Protection: Towards humane social work with families. Bristol: Policy Press.
Figley C (1995) ‘Compassion fatigue as secondary traumatic stress disorder: An overview’, in Figley C (ed) Compassion Fatigue: Coping with secondary traumatic stress disorder in those who treat the traumatized. New York: Brunner-Routledge.
Filipas H and Ullman S (2006) ‘Child sexual abuse, coping responses, self-blame, posttraumatic stress disorder and adult revictimization’, Journal of Interpersonal Violence, 21 (5) 652-672.
Finkelhor D (1979) Sexually Victimized Children. New York: Free Press.
Finkelhor D (1984) Child Sexual Abuse: New theory and research. New York: Free Press.
Firmin C (2013) ‘Something old or something new: Do pre-existing conceptualisations of abuse enable a sufficient response to abuse in young people’s relationships and peer groups?’, in Melrose M and Pearce J (eds) Critical Perspectives on Child Sexual Exploitation and Related Trafficking. Basingstoke: Palgrave Macmillan.
Fleming J (2013) ‘Young people’s participation – Where next?’, Children & Society, 27 (6) 484-495.
Flowe H, Shaw S, Nye E and Jamel J (2009) ‘Rape stereotyping and public delusion’, British Journalism Review, 20 (4) 21-25.
Formby E, Hirst J, Owen J and Hayter M (2011) ‘Barriers to the delivery of school-linked sexual health services in the UK: The influence of societal and school views on young people’s sexual health,’ Journal of Sexual Medicine, 8 (s3).
Fox C (2016) It’s Not on the Radar: The hidden diversity of children and young people at risk of sexual exploitation in England. Ilford: Barnardo’s.
Fox J (2011) Effective Supervision: Using supervision to promote excellent outcomes and enable staff development. Cockermouth: Child Centred Practice.
Franklin A, Raws P and Smeaton E (2015) Unprotected, Overprotected: Meeting the needs of young people with learning disabilities who experience, or are at risk of, sexual exploitation. Ilford: Barnardo’s.
Gagne M, Lavoie F and Hébert M (2005) ‘Victimization during childhood and revictimization in dating relationships in adolescent girls’, Child Abuse and Neglect, 29 (10) 1155-72.
Gibbs J (2001) ‘Maintaining front-line workers in child protection: A case for refocusing supervision’, Child Abuse Review, 10 (5) 323- 335.
Gilbert N, Parton N and Skiveness M. (2011) ‘Changing patterns of responses and emerging orientations’, in Gilbert N, Parton N and Skiveness M (eds) Child Protection Systems: International trends and orientations. Oxford: Oxford University Press.
Giller E (1999) ‘What is psychological trauma?’, workshop presentation (May) at the at ‘Passages to Prevention: Prevention across life’s spectrum,’ Mental Hygiene Administration, Brooklandville, MD.
Gillham J, Reivich K, Freres D, Chaplin T, Shatté A, Samuels B, et al (2007) ‘School-based prevention of depressive symptoms: A randomized controlled study of the effectiveness and specificity of the Penn Resiliency Program’, Journal of Consulting and Clinical Psychology, 75 (1) 9-19.
Gladman A and Heal A (2017) Child Sexual Exploitation after Rotherham: Understanding the consequences and recommendations for practice. London: Jessica Kingsley Publishers.
Glover J (2009) Bouncing back: How can resilience be promoted in vulnerable children and young people? Ilford: Barnardo’s.
Grant L and Kinman G (2016) Building Emotional Resilience in the Children and Families Workforce – An evidence-informed approach. Strategic briefing. Dartington: Research in Practice.
Green R, Rodger H, Cappleman S and Dale R (2014) Learning from Cafcass Submissions to SCRs. November 2014. London: Children and Family Court Advisory and Support Service.
Griffiths S (2013) The Overview Report of the Serious Case Review in Respect of Young People 1,2,3,4,5 & 6. Rochdale: Rochdale Borough Safeguarding Children Board.
Guy J, Feinstein L and Griffiths A (2014) Early Intervention in Domestic Violence and Abuse. Early Intervention Foundation.
Hackett S (2014) Children and Young People with Harmful Sexual Behaviours. Dartington: Research in Practice.
Hackett S (2016) Exploring the Relationship between Neglect and Harmful Sexual Behaviours in Childhood and Adolescence: An evidence scope. Dartington: Action for Children, NSPCC and Research in Practice.
Hallett S (2013) ‘Child Sexual Exploitation’ in South-East Wales: Problems and solutions from the perspectives of young people and professionals’. PHD Thesis, Cardiff University.
Hallett S (2015) Child Sexual Exploitation: Problems and solutions from the perspectives of young people and professionals. (CASCADE research briefing.) Cardiff: Children’s Social Care Research and Development Centre.
Hallett S (2017) Making Sense of Child Sexual Exploitation: Exchange, abuse and young people. Bristol: Policy Press.
Hanson E (2016) Exploring the Relationship between Neglect and Child Sexual Exploitation: An evidence scope. Dartington: Action for Children, NSPCC and Research in Practice.
Hanson E and Holmes D (2014) That Difficult Age: Developing a more effective response to risks in adolescence. Dartington: Research in Practice.
Hardy R (2016) ‘Child exploitation, radicalisation and trafficking: the key questions’, The Guardian, 7 March.
Harper K, Stalker C, Palmer S and Gadbois S (2007) ‘Adults traumatized by child abuse: What survivors need from community-based mental health professionals’, Journal of Mental Health, 17 (4) 361-374.
Hart R (1992) Children’s Participation from Tokenism to Citizenship. Florence: Unicef.
Heath N, Lynch S, Fritch A, McArthur L and Smith S (2011) ‘Silent survivors: Rape myth acceptance in incarcerated women’s narratives of disclosure and reporting of rape’, Psychology of Women Quarterly, 35 (4) 596-610.
Hickle K, Lefevre M, Luckock B and Ruch G (2017) Piloting and Evaluating the ‘See Me, Hear Me’ Framework for working with Child Sexual Exploitation. Final report. Brighton: University of Sussex.
Hicks L and Stein M (2010) Neglect Matters. A multi-agency guide for professionals working together on behalf of teenagers. London: Department for Children, Schools and Families.
HM Government (2015a) Working Together to Safeguard Children: A guide to inter-agency working to safeguard and promote the welfare of children. (This was updated in February 2017 to take account of the revised definition of CSE.) London: Department for Education.
HM Government (2015b) Tackling Child Sexual Exploitation. London: Cabinet Office.
HM Government (2015c) What to do if you’re Worried a Child is being Abused: Advice for practitioners. DFE.
Hoffmann D and Tarzian A (2001) ‘The girl who cried pain: A bias against women in the treatment of pain’, Journal of Law, Medicine and Ethics, 28 (Supplement s4) 13-27.
Home Office (2015) This is Abuse Campaign: Summary report. London: Home Office.
Horvath M, Alys L, Massey K, Pina A, Scally M and Adler J (2013) ‘Basically…porn is everywhere’: A rapid evidence assessment on the effect that access and exposure to pornography has on children and young people. London: Office of the Children’s Commissioner.
House of Commons Education Committee (2015) Life lessons: PSHE and SRE in schools: Fifth Report of Session 2014–15. London: House of Commons.
Jago S, Arocha L, Brodie I, Melrose M, Pearce J and Warrington C (2011) What’s Going On to Safeguard Children and Young People from Sexual Exploitation? How local partnerships respond to child sexual exploitation. Luton: University of Bedfordshire.
James A and Prout A (1997) Constructing and Reconstructing Childhood: Contemporary Issues in the Sociological Study of Childhood (2nd edition), London: Falmer.
James A, Winmill L, Anderson C and Alfoadari K (2011) ‘A preliminary study of an extension of a community Dialectic Behaviour Therapy (DBT) programme to adolescents in the looked after care system’, Child and Adolescent Mental Health, 16 (1) 9-13.
Jay A (2014) Independent Inquiry into Child Sexual Exploitation in Rotherham: 1997-2013. Rotherham: Rotherham Metropolitan Borough Council.
Johnson R and Cotmore D (2015) National Evaluation of the Graded Care Profile. London: NSPCC.
Jonas S, Bebbington P, McManus S, Meltzer J, Jenkins R, Kuipers E et al (2011) ‘Sexual abuse and psychiatric disorder in England: results from the 2007 Adult Psychiatric Morbidity Survey’, Psychological Medicine, 41(4) 709-19.
Jones R (2014) The Story of Baby P: Setting the record straight. Bristol: Policy Press.
Kaestle C (2012) ‘Selling and buying sex: A longitudinal study of risk and protective factors in adolescence’, Prevention Science, 13 (3) 314-322.
Kelly L (1988) Surviving Sexual Violence. Cambridge: Polity Press.
Kelly L, Wingfield R, Burton S and Regan L (1995) Splintered Lives: Sexual exploitation of children in the context of children’s rights and child protection. Ilford: Barnardo’s.
Kelly P (2003) ‘Growing up as risky business? Risks, surveillance and the institutionalized mistrust of youth’, Journal of Youth Studies, 6 (2) 165-180.
Khoo E, Hyvönen U and Nygren L (2002) ‘Child welfare or child protection: Uncovering Swedish and Canadian orientations to social intervention in child maltreatment’, Qualitative Social Work, 1 (4) 451-71.
Khwali J, Martin L, Brady G and Brown S (2016) ‘Child sexual abuse and exploitation: Knowledge, confidence and training within a contemporary UK social work practice and policy context’, British Journal of Social Work, 46 (8) 2208-2226.
Kinman G and Grant L (2011) ‘Exploring stress resilience in trainee social workers: The role of social and emotional competence’, British Journal of Social Work, 41 (2) 261-75.
Kirby D, Laris B and Rolleri L (2007) ‘Sex and HIV education programs: Their impact on sexual behaviors of young people throughout the world’, Journal of Adolescent Health, 40 (3) 206-217.
Kohler P, Manhart L and Lafferty W (2008) ‘Abstinence-only and comprehensive sex education and the initiation of sexual activity and teen pregnancy’, Journal of Adolescent Health, 42 (4) 344-351.
Lalor K and McElvaney R (2010) ‘Child sexual abuse, links to later sexual exploitation/high-risk sexual behavior, and prevention/ treatment programs’, Trauma, Violence, & Abuse, 11 (4) 159-177.
Laming H (2003) The Victoria Climbié Inquiry: Report. London: The Stationery Office.
Laming H (2009) The Protection of Children in England: A progress report. London. House of Commons.
Lebloch E and King S (2006) ‘Child sexual exploitation: A partnership response and model intervention’, Child Abuse Review, 15 (5) 362- 372.
Lemos G (2009) Freedom’s Consequences: Reducing teenage pregnancies and their negative effects in the UK. London: Lemos & Crane.
Lerner M (1980) The Belief in a Just World: A fundamental delusion. (Perspectives in Social Psychology.) New York: Springer Science.
Linehan M (1993) Cognitive Behavioural Treatment of Borderline Personality Disorder. New York: Guilford.
Local Government Association (2014) Tackling Child Sexual Exploitation: A resource pack for councils. London: LGA.
Lodrick Z (2007) ‘Psychological trauma – What every trauma worker should know’, The British Journal of Psychotherapy Integration, 4 (2) 18-28.
London Assembly (2015) Confronting Child Sexual Exploitation in London. London: Greater London Authority.
London K, Brook M, Ceci S and Shuman D (2005) ‘Disclosure of child sexual abuse: What does the research tell us about the ways that children tell?’, Psychology, Public Policy, and Law, 11 (1) 194-226.
Macdonald G, Higgins J, Ramchandani P, Valentine J, Bronger L, Klein P et al (2012) ‘Cognitive-behavioural interventions for children who have been sexually abused: A systematic review’, Campbell Systematic Reviews 2012:14, DOI: 10.4073/csr.2012.14.
Macdonald G, Lewis J, Macdonald K, Gardner E, Murphy L, Adams C et al (2014) ‘The SAAF Study: Evaluation of the Safeguarding Children Assessment and Analysis Framework (SAAF), compared with management as usual, for improving outcomes for children and young people who have experienced, or are at risk of, maltreatment: Study protocol for a randomized controlled trial’, Trials 15 (1) 453.
Marshall L and Marshall W (2016) ‘The treatment of adult male sex offenders’, in Boer D (ed) The Wiley Handbook of Theories, Assessment and Treatment of Sexual Offending: Volume III Treatment. John Wiley and Sons.
Martellozzo E, Monaghan A, Adler J, Davidson J, Leyva R and Horvath M (2016) “…I wasn’t sure it was normal to watch it…” (Revised May 2017). London: NSPCC.
Martin L, Brady G, Kwhali J, Crowe S and Matouskova G (2014) Social Workers’ Knowledge and Confidence when Working with Cases of Child Sexual Abuse: What are the issues and challenges? London. NSPCC.
Mason G, Ullman S, Long S, Long L and Starzynski S (2008) ‘Social support and risk of sexual assault revictimization’, Journal of Community Psychology, 37 (1) 58-72.
Mayock P, Kitching K and Morgan M (2007) RSE in the Context of SPHE: An assessment of the challenges to full implementation of the programme in post-primary schools. Dublin: Crisis Pregnancy Agency/Dept of Education and Science.
McMahon S and Farmer L (2011) ‘An updated measure for assessing subtle rape myths’, Social Work Research, 35 (2) 71-81.
McNeish D and Scott S (2014) Women and Girls at Risk: Evidence across the life course. London: LankellyChase Foundation.
McNeish D and Scott S (2015) An independent evaluation of Rape Crisis Scotland’s sexual violence prevention project: Final report. Rape Crisis Scotland.
Medforth R (2011) Family Work at SCARPA: Parents’ views and experiences. Leeds: The Children’s Society.
Medina J, Cebulla A, Ross A, Shute J and Aldridge J (2013) Children and Young People in Gangs: A longitudinal analysis. Summary and policy implications. London: Nuffield Foundation.
Melrose M (2013) ‘Twenty-first century party people: Young people and sexual exploitation in the new millennium’, Child Abuse Review, 22 (3) 155-168.
Miller A, Markman K and Handley I (2007) ‘Self-blame among sexual assault victims prospectively predicts revictimization: A perceived sociolegal content model of risk’, Basic and Applied Psychology, 29 (2) 129-136.
Ministry of Justice, Home Office and Office for National Statistics (2013) An Overview of Sexual Offending in England and Wales. London: MoJ.
Minuchin S (1974) Families and Family Therapy. London: Tavistock.
Möller A, Söndergaard H and Helström L (2017) ‘Tonic immobility during sexual assault – A common reaction predicting post-traumatic stress disorder and severe depression’. AOGS: Acta Obstetrica et Gynecologica Scandinavica, 96 (8) 932-938.
Moran P, Jacobs C, Bunn A and Bifulco A (2007) ‘Multi-agency working: Implications for an early-intervention social work team,’ Child and Family Social Work, 12 (2) 143–151.
Morrison T (2001) Staff Supervision in Social Care. Brighton: Pavilion.
Morrison T (2005) Staff Supervision in Social Care: Making a real difference for staff and service users. (3rd edition.) Brighton: Pavilion.
Moshman D (2011) ‘Adolescents and their teenage brains’, Human Development, 54: 201-203.
Munro E (2011) The Munro Review of Child Protection: Final report. A child-centred system. London: Department for Education.
NatCen (2014) Violence, Abuse and Mental Health in England: Preliminary evidence briefing. London: NatCen Social Research. National Working Group (2010) A National Picture of Child Sexual Exploitation and Specialist Provisions in the UK. London: NWG.
National Working Group (2015) What is Child Sexual Exploitation? London: NWG.
National Youth Agency (2004) Ethical Conduct in Youth Work: A statement of values and principles from The National Youth Agency. Leicester: NYA.
Nelson E, Heath A, Madden P, Cooper M, Dinwiddie S and Bucholz K et al (2002) ‘Association between self-reported childhood sexual abuse and adverse psychosocial outcomes: Results from a twin study’, Archives of General Psychiatry, 59 (2) 139-45.
NESTA (2013) By Us, For Us: The power of co-design and co-delivery. London: Nesta.
Newman T (2004) What Works in Building Resilience? Ilford: Barnardo’s.
NICE (2010) Review of Personal, Social, Health and Economics (PSHE) Education. (NICE response to the Department for Education review of PSHE.)
NSPCC (2013a) Child sexual exploitation: Learning from case reviews. Summary of risk factors and learning for improved practice around CSE. NSPCC.
NSPCC (20013b) Child Sexual Abuse: An overview of the current literature on child sexual abuse. An NSPCC research briefing. NSPCC.
NSPCC (2013c) Vicarious Trauma: The consequences of working with abuse. An NSPCC research briefing. NSPCC.
O’Connell R (2003) A Typology of Cybersexploitation and Online Grooming Practices. Preston: University of Central Lancashire, Cyberspace Research Unit.
O’Connell Davidson J (2005) Children in the Global Sex Trade. Cambridge: Polity Press.
Office of the Children’s Commissioner (2012) ‘I thought I was the only one. The only one in the world.’ The Office of the Children’s Commissioner’s Inquiry into Child Sexual Exploitation In Gangs and Groups. Interim report. London: OCC.
Office of the Children’s Commissioner (2013a) ‘If only someone had listened.’ Office of the Children’s Commissioner’s Inquiry into Child Sexual Exploitation in gangs and groups. Final report.
Office of the Children’s Commissioner (2013b) Participation Strategy: May 2013 – April 2014. London: OCC.
Office of the Children’s Commissioner (2017) On Measuring the Number of Vulnerable Children in England. London: OCC.
Ofsted (2010) Learning from Serious Case Reviews 2009-2010. Manchester: Ofsted.
Ofsted (2013) Effective Professional Development in Youth Services: Bath and North East Somerset Council. Good practice example. Manchester: Ofsted.
Ofsted (2014) The Sexual Exploitation of Children: It couldn’t happen here, could it? Manchester: Ofsted.
Ofsted (2105) The Quality of Assessment for Children in Need of Help. Manchester: Ofsted.
PACE (2013) Are Parents in the Picture? Professional and parental perspectives of child sexual exploitation. Leeds: Pace and Virtual College’s Safeguarding Children e-Academy.
PACE (2014) The Relational Safeguarding Model: Best practice in working with families affected by child sexual exploitation. Leeds: Parents Against Child Sexual Exploitation (PACE).
Palmer T (2015) Digital Dangers: The impact of technology on the sexual abuse and exploitation of children and young people. Ilford: Barnardo’s and the Marie Collins Foundation. Barnardo’s.
Park B, Wilson G, Berger J, Christman M, Reina B, Bishop F et al (2016) ‘Is internet pornography causing sexual dysfunctions? A review with clinical reports’, Behavioural Sciences, 6 (3) 17, DI: 10.3390/bs6030017.
Parton N (2014) The Politics of Child Protection: Contemporary developments and future directions. London: Palgrave Macmillan.
Payne D, Lonsway K and Fitzgerald L (1999) ‘Rape myth acceptance: Exploration of its structure and its measurement using the Illinois Rape Myth Acceptance Scale.’ Journal of Research in Personality, 33, 27–68. DOI:10.1006/jrpe.1998.2238.
Pearce J (2009a) Young People and Sexual Exploitation: ‘It’s not hidden, you just aren’t looking’. Abingdon: Routledge.
Pearce J (2009b) ‘Beyond child protection: Young people, social exclusion and sexual exploitation’, in Phoenix J (ed) Regulating Sex for Sale: Prostitution policy reform in the UK. Bristol: Policy Press.
Pearce J (2009b) ‘Beyond child protection: Young people, social exclusion and sexual exploitation’, in Phoenix J (ed) Regulating Sex for Sale: Prostitution policy reform in the UK. Bristol: Policy Press.
Pearce J (2014) ‘What’s going on to safeguard children and young people from child sexual exploitation: A review of Local Safeguarding Children Boards’ work to protect children from sexual exploitation’, Child Abuse Review, 23 (3) 159-170.
Phoenix J (2002) ‘In the name of protection: Youth prostitution policy reforms in England and Wales’, Critical Social Policy, 22 (2) 353- 375.
Pincus A and Minahan A (1973) Social Work Practice: Model and method. Illinois: F.E. Peacock Publishers.
Pona I, Royston S, Bracey C and Gibbs A (2015) Seriously Awkward: How vulnerable 16–17 year olds are falling through the cracks. London: The Children’s Society.
Project Phoenix (2014) Project Phoenix Handbook: Multi-agency guidance for delivering effective strategies to tackling child sexual exploitation in Greater Manchester. Manchester: Project Phoenix.
Quadara A and Hunter C (2016) Principles of Trauma-informed Approaches to Child Sexual Abuse: A discussion paper. Sydney: Royal Commission into Institutional Responses to Child Sexual Abuse.
Radford L, Corral S, Bradley C, Fisher H, Bassett C, Howat N and Collishaw S (2011) Child Abuse and Neglect in the UK Today. NSPCC, London.
Rainer (now Catch22) (2008) Developing Your Pledge to Children and Young People. Part of the What Makes the Difference? Project.
Read D (2002) ‘A multitrajectory, competition model of emergent complexity in human social organization’, Proceedings of the National Academy of Sciences of the United States of America, 99, Supplement 3 (14th May), pp. 7251-7256, DOI: 10.1073/pnas.072079999
Rees G and Stein M (1999) The Abuse of Adolescents within the Family. London: NSPCC.
Reid J (2011) ‘An exploratory model of girls’ vulnerability to commercial sexual exploitation in prostitution’, Child Maltreatment, 16 (2) 146-157
Rekart M (2005) ‘Sex-work harm reduction’, The Lancet, December 17; 366 (9503): 2123-2134.
Research in Practice (2014a) Analysis and Critical Thinking in Assessment. (2nd edition.) Dartington: Research in Practice.
Research in Practice (2014b) Promoting Resilience in Children, Young People and Families: Frontline briefing. (Updated) Dartington: Research in Practice.
Research in Practice (2014c) Supporting Emotional Resilience within Social Workers. Dartington: Research in Practice. Research in Practice (2016a) Violence in Young People’s Relationships. Frontline briefing. Dartington: Research in Practice.
Research in Practice (2016b) Attachment in children and young people: Frontline briefing. (Updated) Dartington: Research in Practice.
Research in Practice (2017) Young Person-centred Approaches in Child Sexual Exploitation (CSE) – Promoting participation and building self-efficacy. Frontline briefing. Dartington: Research in Practice.
Ringrose J, Gill R, Livingstone S and Harvey L (2012) A Qualitative Study of Children, Young People and ‘Sexting’: A report prepared for the NSPCC. London: NSPCC.
Ringrose J, Harvey L, Gill R and Livingstone S (2013) ‘Teen girls, sexual double standards and ‘sexting’: Gendered value in digital image exchange’, Feminist Theory, 14 (3) 305-323.
Rizvi S, Steffel L, and Carson-Wong A (2013) ‘An overview of dialectical behaviour therapy for professional psychologists’, Professional Psychology: Research and Practice, 44 (2) 73-80.
Rogstad K and Johnston G (2014) Spotting the Signs: A national proforma for identifying risk of child sexual exploitation in sexual health services. Macclesfield: BASHH (British Association for Sexual Health and HIV) and Brook.
Romer D (2010) ‘Adolescent risk taking, impulsivity, and brain development: Implications for prevention’, Developmental Psychobiology, 52 (3) 263–276.
Royal College of General Practitioners and NSPCC (2014) Safeguarding Children and Young People: The RCGP/NSPCC Safeguarding Children Toolkit for General Practice. London: RCGP.
Royal College of Nursing (2014) An RCN toolkit for School Nurses: Developing your practice to support children and young people in educational settings. London: RCN.
Safeguarding Board Northern Ireland (2014) Child Sexual Exploitation: Definition and guidance. Belfast: SBNI.
Schofield G, Ward E, Biggart L, Scaife V, Dodsworth J, Larsson B et al (2012) Looked after Children and Offending: Reducing risk and promoting resilience. Norwich: University of East Anglia and TACT.
Schrader-McMillan A and Barlow J (2017) Improving the Effectiveness of the Child Protection System – A review of literature. London: Early Intervention Foundation.
SCIE Co-production in Social Care: What it is and how to do it. (Guide 51.)
Scott S and Skidmore P (2006) Reducing the Risk: Barnardo’s support for sexually exploited young people. A two-year evaluation. Ilford: Barnardo’s.
Scott S, Botcherby S and Ludvigsen A (2017) Wigan and Rochdale Child Sexual Exploitation Innovation Project: Evaluation report. London: Department for Education
Scott S and McNeish D (2017) Supporting parents of sexually exploited young people An evidence review. Centre of Expertise on Child Sexual Abuse.
Shaw S, Nye E, Jamel J and Flowe H (2009) ‘The print media and rape’, The Psyhcologist, Vol.22
Shuker L (2013a) ‘Constructs of Safety for Children in Care Affected by Sexual Exploitation’ in Melrose M and Pearce J (eds) Critical Perspectives on Child Sexual Exploitation and Related Trafficking. Palgrave Connect. pp.125-138.
Shuker L (2013b) Evaluation of Barnardo’s Safe Accommodation Project for Sexually Exploited and Trafficked Young People. Luton: University of Bedfordshire.
Shuker L (2015) ‘Definitions of abuse: A contemporary context’, workshop presentation, December 2015
Skuse D, Bentovim A, Hodges J, Stevenson J, Andreou C, Lanyado M et al (1998) ‘Risk factors for the development of sexually abusive behaviour in sexually victimised adolescent males: cross sectional study’, BMJ, 317 (7152) 175-9.
Smeaton E (2013a) Working with Children and Young People who Experience Running Away and Child Sexual Exploitation: An evidence- based guide for practitioners. Ilford: Barnardo’s.
Smeaton E (2013b) Running from Hate to what you Think is Love: The relationship between running away and child sexual exploitation. Barnardo’s.
Smeaton E (2014) ‘Keep Doing what you’re Doing’: Evaluation Findings of Checkpoint’s Sexual Exploitation Live Freely Project. The Children’s Society.
Smeaton E, Franklin A and Raws P (2015) Practice Guide: Supporting professionals to meet the needs of young people with learning disabilities who experience, or are at risk of, child sexual exploitation. Ilford: Barnardo’s.
Smith C, Stainton R and Tucker S (2007) ‘Risk’, in Robb M (ed) Youth in Context: frameworks, settings and encounters. London: Sage/ Open University.
Smith M (2002) ‘Transforming youth work – Resourcing excellent youth services. A critique’.
Squires P and Stephen D (2005) ‘Rougher justice: Anti-social behaviour and young people’, British Journal of Social Work, 36 (2) 349- 351.
Srivastava O and Polnay L (1997) ‘Field trial of graded care profile (GCP) scale: A new measure of care’, Archives of Disease in Childhood, 76 (4) 337-40.
Stanley N (2011) Children Experiencing Domestic Violence: A research review. Dartington: Research in Practice.
Stevens I and Cox P (2008) ‘Complexity theory: Developing new understandings of child protection in field settings and in residential child care’, British Journal of Social Work, 38 (7) 1320-1336.
Stevens I and Hassett P (2007) ‘Applying complexity theory to risk in child protection practice’, Childhood, 14 (1) 129-146.
Stevenson L (2014) ‘It’s easier that way”: Why a third of child sexual exploitation victims are overlooked’.
Stewart A and Thompson C (2004) Comparative Evaluation of Child Protection Assessment Tools. Queensland: Griffith University.
Sturrock R and Holmes L (2015) Running the Risks: The links between gang involvement and young people going missing. London: Catch22.
Surrey County Council and FutureGov (2014) A Rough Guide to the Shift Surrey Approach.
Taylor-Browne J (2002) More Than One Chance: Young people involved in prostitution speak out. London: ECPAT UK.
Terrence Higgins Trust (2016) Shh…No Talking: LGBT-inclusive sex and relationships education in the UK. London: Terrence Higgins Trust.
Thompson J (2014) Reaching Safe Places: Exploring the journeys of young people who run away from home or care. Railway Children.
Thornberry T, Henry K, Ireland T and Smith C (2010) ‘The causal impact of childhood-limited maltreatment and adolescent maltreatment on early adult adjustment,’ Journal of Adolescent Health, 46 (4) 359-365.
Tisdall K (2008) ‘Is the honeymoon over? Children and young people’s participation in public decision-making’, International Journal of Children’s Rights, 16 (3) 419-429.
Trask E, Walsh K and DiLillo D (2010) ‘Treatment effects for common outcomes of child sexual abuse: A current meta-analysis’, Aggression and Violent Behavior. 16 (1) 6–19. DOI: 10.1016/j.avb.2010.10.001
Turney D, Platt D, Selwyn J and Farmer E (2011) Social Work Assessment of Children in Need: What do we know? Messages from research. London: Department for Education.
Ullman S and Vasquez A (2015) ‘Mediators of sexual revictimization risk in adult sexual assault victims’, Journal of Child Sexual Abuse, 24 (3) 300-314.
Van Leijenhorst L, Zanolie K, Van Meel C, Westenberg P, Rombouts S and Crone E (2010) ‘What motivates the adolescent? Brain regions mediating reward sensitivity across adolescence’, Cerebral Cortex, 20 (1) 61-69.
van Loon A and Kralik D (2005a) Facilitating Transition after Child Sexual Abuse. Glenside, S. Aust: Royal District Nursing Service Foundation Research Unit.
van Loon A and Kralik D (2005b) Reclaiming Myself after Child Sexual Abuse. Glenside, S. Aust: Royal District Nursing Service Foundation Research Unit.
Villani S (2003) ‘Media violence: More than just child’s play?’ Facts of Life: Issue Briefings for Health Reporters, Vol. 8, No. 10.
Vosmer S, Hackett S and Callanan M (2009) ‘“Normal” and “inappropriate” childhood sexual behaviours: Findings from a Delphi study of professionals in the United Kingdom’, Journal of Sexual Aggression, 15 (3) 275-288.
Wallbank S and Wonnacott J (2015) ‘The integrated model of restorative supervision for use within safeguarding’, Community Practitioner. 88 (5) 41-45.
Ward T and Beech A (2006) ‘An integrated theory of sexual offending’, Aggression and Violent Behavior, 11 (1) 44-63.
Warrington C (2016) ‘Child sexual exploitation: young people’s perspectives on professional support’, practice guidance.
Wastell D and White S (2012) ‘Blinded by neuroscience: Social policy, the family and the infant brain’, Families, Relationships and Societies, 1 (3) 397-414
Wethington H, Hahn R, Fuqua-Whitley D, Sipe T, Crosby A, Johnson R et al (2008) ‘The effectiveness of interventions to reduce psychological harm from traumatic events among children and adolescents’, American Journal of Preventive Medicine, 35 (3) 287–313.
Whittle H, Hamilton-Giachritsis C, Beech A and Collings G (2013) ‘A review of young people’s vulnerabilities to online grooming’, Aggression and Violent Behavior, 18 (1) 62-70. DOI: 10.1016/j.avb.2012.09.003.
Williams J and Keating F (2002) ‘The abuse of adults in psychiatric settings’, in Stanley N, Manthorpe J and Penhale B (eds) Institutional Abuse: Perspectives across the life course. London: Routlegde.
Williams J and Watson G (2016) ‘Surviving their lives: Women’s mental health in context’, in Castle D and Abel K (eds) Comprehensive Women’s Mental Health. Cambridge: Cambridge University Press.
Wiseman J and Davies E (2013) Recruitment, Retention and Career Progression of Social Workers. (Report for the Local Government Association.) BMG Research.
Wolak J, Finkelhor D, Mitchell K and Ybarra M (2008) ‘Online “predators” and their victims: Myths, realities, and implications for prevention and treatment’, American Psychologist, 63 (2) 111-128.
Womankind Worldwide (2010) Freedom to achieve. Preventing violence, promoting equality: A whole-school approach. London: Womankind Worldwide.
Women and Equalities Committee (2016) Sexual Harassment and Sexual Violence in Schools. London: House of Commons.
Wonnacott J (2012) Mastering Social Work Supervision. London: Jessica Kingsley Publishers.
World Health Organization (2013) Global and Regional Estimates of Violence Against Women: Prevalence and health effects of intimate partner violence and non-partner sexual violence. Geneva: World Health Organization.
Wurtele S and Miller-Perrin C (1992) Preventing Sexual Abuse: Sharing the Responsibility. Lincoln, NE: University of Nebraska Press.
Yi J (2015) ‘The role of benevolent sexism in gender inequality’, New York University, Department of Applied Psychology, OPUS (Online Publication of Undergraduate Studies)
Yorkshire MESMAC (2015) Excellence for Boys Project: Summary of initial findings. Leeds: Yorkshire MESMAC.
Zoldbrod A (2013) ‘Why a sex therapist worries about teens viewing internet porn’, Common Health.
Professional Standards
PQS:KSS - Relationships and effective direct work | Abuse and neglect of children | Child and family assessment | Analysis, decision-making, planning and review | Developing excellent practitioners | Shaping and influencing the practice system | Confident analysis and decision-making | Purposeful and effective social work | Emotionally intelligent practice supervision | Designing a system to support effective practice | Developing excellent practitioners
PCF - Knowledge | Intervention and skills